 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 2, 2004, pp. 52-54 CASE REPORT TUBEROUS SCLEROSIS AND ACUTE HYDROCEPHALUS Nebi Yılmaz1, Nejmi Kıymaz1, Cahide Yılmaz2, Ömer Çalka3, Ömer Etlik4, Taner Yazıcı1 Yuzuncu Yıl University, Faculty of Medicine, Departments of Neurosurgery1,
Pediatric Neurology2, Dermatology3 and
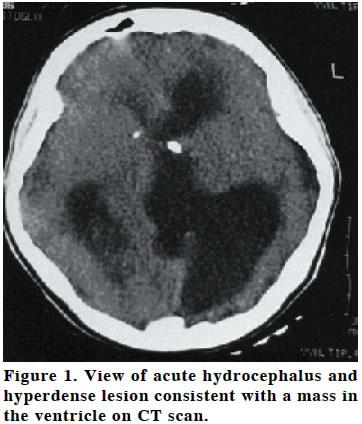
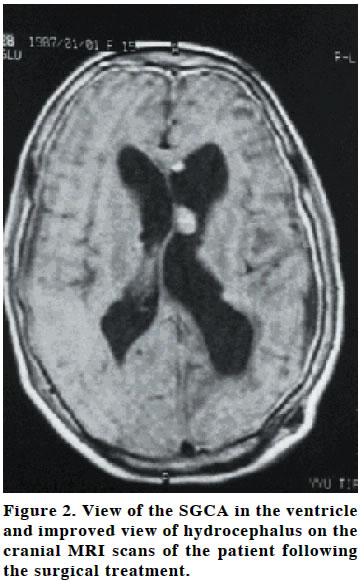
Radiology4 Code Number: gm04022 Tuberous sclerosis complex is a neurocutaneous and autosomal dominant disease characterized by multiple hamartomas in multiple viscera. It results from spontaneous mutation. The genetic anomaly is usually linked to the 9th chromosome. It may be accompanied by early childhood seizures, multiple brain tumors, skin lesions, angiomyolipomas in the kidneys and liver and rhabdomyomas. A careful physical examination, computerized tomography (CT) and magnetic resonance imaging (MRI) scans of the brain are essential in its diagnosis. In this study, we presented a 16 year old girl who was brought to our emergency service room due to acute loss of conscious and then underwent to ventriculo-peritoneal (V-P) shunt procedure after she had been diagnosed as acute hydrocephalus. The patient had been operated for intracranial mass when she was 2 years old and postoperative pathological diagnosis was established to be subepandimal giant cell astrocytoma (SGCA). Key words: Tuberous sclerosis, Subepandimal giant cell astrocytoma INTRODUCTION Tuberous sclerosis complex (TSC) was first defined in 1862 by Von Recklinghausen. In 1880, Bourneville proposed the term “tuberous sclerosis”because of the relationship of the disease with mental retardation, epilepsy and cortical tubers. Its incidence has been estimated to be 1:10.000 to 1:70.000 in neonates. Its pathognomonic findings are angiofibroma on the face, cortical tuber, subepandimal nodules or SGCA, multiple retinal astrocytoma and multiple subepandimal nodules extending into the ventricle. SGCA develops from the growth of subepandimal nodules. These tumors typically arise from terminal sulcus location adjacent to foramen monro. They usually lead to obstructive hydrocephalus and increased frequency of epileptic seizures. Cranial CT and MRI scanning are important in its diagnosis (1-3). Our purpose in this case is to emphasize that SGCAs in tuberosclerosis complex, especially due to involvement around the foramen magnum may constitute a potential pathology for acute hydrocephalus. CASE A 16-years-old girl was brought to our emergency service for acute loss of conscious and epileptic seizure. Brain CT obtained in emergency setting revealed acute hydrocephalus and the patient underwent to emergency ventriculo-peritoneal shunt (V-P) operation. The patient’s history revealed that she had gone to another medical center for epileptic seizure when she was 2 years old and investigations revealed that she had had intracranial mass. She had underwent intracranial mass excision and pathological examination of operation material had revealed SGCA. A mass lesion of 1.5x0.5 cm in the location of foramen monro anterior to septum pellucidum of the horn of the left lateral ventricle (consistent with giant cell astrocytoma) and lesions of multiple tuberosclerosis in the cortical areas were seen on the MRI scans of the patient. The skin lesions of the patient were considered as consistent with tuberosclerosis but no ophthalmic, cardiac or renal pathology was found. General health status of the patient improved after the V-P shunt. No serious problem developed during the follow-up of the patient for 1 year. DISCUSSION Tuberous sclerosis is a neurocutaneous syndrome characterized by hamartomas in a number of viscera. Takanashi et al. (1) proposed that half of the cases were autosomal dominant and the other half them were sporadic cases and suggested that the genes TSC1 and TSC2 might be responsible for these cases. Hamartomas are benign lesions although they rarely may show malign progression. Subepandimal giant cell astrocytoma is a slow-growing glial tumor (4). SGCAs are distinguished from other astrocytomas with their non-invasive nature and the fact that almost all of them locate in the ventricle (5,6). Spontaneous regression has not been observed in SGCAs. Curatolo et al. (3) reported that astrocytic astrocytoma regressed in a patient with Tuberosclerosis complex. Although rare, SGCAs may have such histological malignancy criteria as necrosis, mitosis and vascular proliferation. Kashiwagi et al. (2) reported a patient with SGCA only without any pathology in other systems. Mortality in tuberous sclerosis is due to cardiac, renal and cerebral pathologies. Sudden deaths may be seen following cardiac arrhythmias, epilepsy, intracranial hemorrhages, obstructive hydrocephalus, aneurism rupture and spontaneous pneumothorax (7,8). SGCAs most commonly develop especially around the foramen magnum. Thus, they may lead to sudden deaths due to acute hydrocephalus (9). Hence, the patients with SGCA should be followed closely for hydrocephalus after the surgical procedure because of the importance of location of the tumor. The patient presented in this paper developed acute hydrocephalus due to growth of the mass 14 years after she had been operated. In conclusion, in our opinion V-P shunt would be appropriate for hydrocephalus which may develop even though SGCT is not within surgical margins. We suggest that the patient should be followed closely or underwent V-P shunt for hydrocephalus if surgical treatment has been performed. REFERENCE
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04022f1.jpg] [gm04022f2.jpg] |
| |||||||||

{kind=link}
{kind=link}