 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 2, 2004, pp. 55-58 CASE REPORT MYOCARDIAL INFARCATION IN A YOUNG PATIENT WITH HIGH HDL-CHOLESTEROL LEVEL AND NO OTHER RISK FACTORS APART FROM SMOKING Levent Özdemir1, Ali Süner2, Sıddık Ülgen1 Dicle University, Faculty of Medicine, Departments of Cardiology1 and
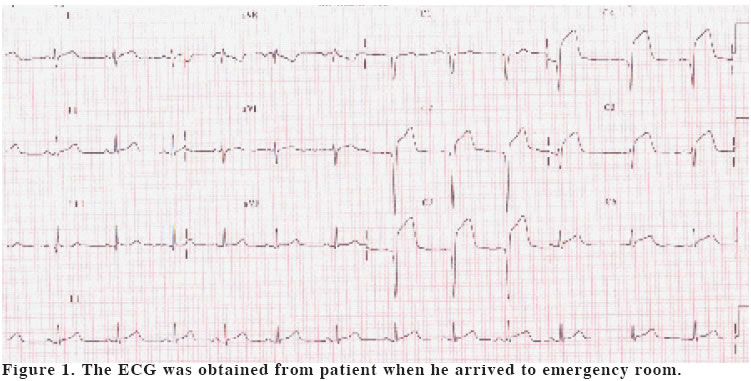
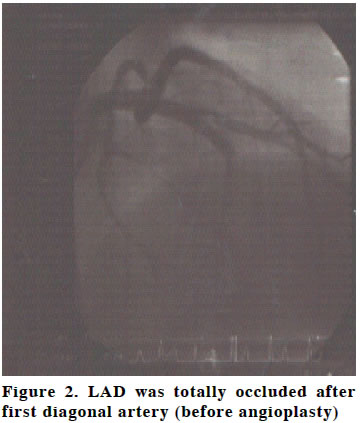
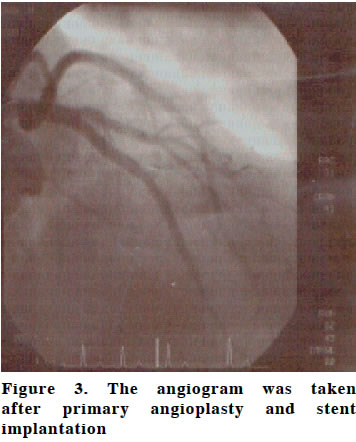
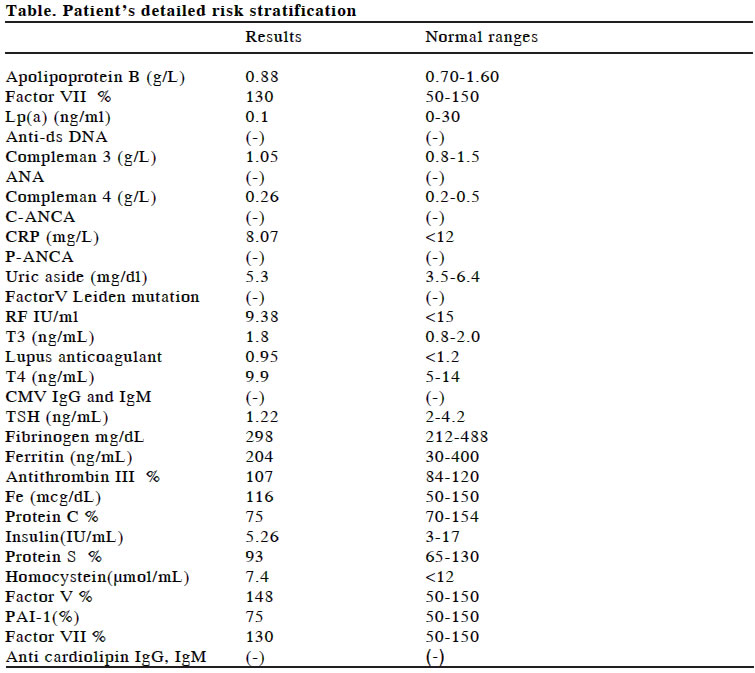
Internal Medicine2, Code Number: gm04022 There is a low incidence of myocardial infarction (MI) for those under 45 years old. Many risk factors have been described for MI. Some risk factors may be especially important for younger people. A 23 year-old young patient with acute anterior myocardial infarction and no prior symptoms was presented. The patient was treated with precutaneous transluminal coronary angioplasty (PTCA). Although we investigated the risk factor in detail. We couldn’t find any risk factors apart from cigarette smoking. The patient had high HDL-cholesterol level and as it is known this eliminate one positive risk factor. The occurence of MI in a patient with high HDL cholesterol who has no other risk factors apart from cigarette smoking is a remarkable sample that cigarette smoking is an extremely important risk factor for young patients and that HDL cholesterol level is not sufficient enough to prevent the negative effects of this risk factor. Key words: Young patient, myocardial infarction, cigarette smoking INTRODUCTION Death rate due to coronary heart diseases is one of the major death reasons in our country as it is in western societies. Among the reasons of the escalating emergence of CHD (KKH) among the young are; decrease in smoking start age, malnutrition habit, the advent of obesity in earlier ages, lack of exercise and excessive consumption of saturated oil.In the case of this young patient we didn’t face any known risk factors except cigarette smoking in the advent of acute coronary syndrome. In spite of studying many major and newly-researched risk factors ,we couldn’t find any of these (1). We especially wanted to show that cigarette smoking is a very significant risk factor among the young patient group by presenting the case of this young patient who suffered MI due to smoking despite high HDL cholesterol. CASE The 23-year-old male patient with no previous cardiac complaint admitted our emergency service with the complaint of feeling chest pain like straint starting from left arm to dorsal side, after meal.The pain was accompanied with cold sweating, nausea and vomitting. The pain started 4 hours before and was still continuing in the emergency room. In ECG there was QS in the derivations of V1-V4, 3 mm ST elevation in V1-V6, and decrease R wave amplitutue in V5-V6 (Figure 1). The blood pressure was 130/80 and the pulse was 75/bpm and regular. No pathological finding was found in physical examination.The patient was diagnosed acute anterior MI. In the immediate coronary angiography performed through right femoral artery with Judkins technique LAD was totally occluded after first diagonal artery (Figure 2). Balloon dilatation and afterwards due to its suboptimal result, stent implementation were perfomed successfully (Figure 3). Antiagregan, anticoagulant, beta-blocker, nitrate, ACE inhibitor, statin and glicoprotein IIB/IIA receptor inhibitor treatment was given. Of the cardiac enzymes, creatin phosphokinase MB (CK-MB) 643 IU/L (normal<25IU/L) and Troponin-I value >100ng/mL (normal<1.0 ng/mL) were high. The other biochemistry and complete blood count values were normal. Of the blood lipids, total chollestrol was 210 mg/dL, HDL chollestrol 61 mg/dL, LDL-C 139 mg/dL, triglyceride 50 mg/dL. The patient had been smoking 1, 5 packets of cigarette a day for the last 12 years. In the test of echocardiography on the second day, septum and anterior were found to be mid, apikal parts with hypokinetik and the ejection fraction 45%. On the sixth day of his admission, the patient was discharged without any cardiac problem and insufficiency. DISCUSSION Young patients with MI constitute the 4% and 10% of all patients with MI.There are many risk factors in the advent of coronary artery disease (CAD) in young patients. While some of these risk factors are less frequent some are relatively more frequent. Smoking is the most frequently seen risk factor in young patients with MI (2). The amount of smoking is inversely proportional to the age of MI advent.The risk of coronary artery disease in young patients with hypercholesterolemia and no other risk factors increases remarkably (3). The levels of increased triglyceride and low HDL cholesterol have been shown in young patients with MI (3). Positive family history in young patients is a major risk factor of the advent of CAD. Although hypertension is a major risk factor for young patients, it is rarely seen in comparision with adult groups (3). Diabetes Mellitus is the cause of 10% of MIs in young patients. Between 30% and 60% of the youngs with MI have obesity. Today it is known that use of cocaine may cause MI in young patients.It is assumed that high level of homoscystein has effect on endotel and causes proliferation in smooth muscles, also it causes an increase in coronary arter disease. In many studies the correlation between high lipoprotein concentration(a) (lp(a)) and CAD has been shown (3). In some cases where coagulable state increases also, there is an increased risk of CAD. Among these are the high level of factor VII which can increase the production of trombin and result in a condition of hypercoagulability, the lack of antitrombin III which controls the effect of procagulan trombin, and the levels of increased fibrinogen which have been shown as a seperate risk factor.PAI-1 levels in patients with MI before the age of 45 have been found higher when compared with healthy individuals(6). In recent years, with the popularity of the notion that the atherosclerosis associated with inflammation, high level of C reactive protein (CRP) is a risk factor in the advent, development and instability of coronary artery disease . For many years CAD has been claimed to be able to accompany bacterial and viral agents.Chlamidya pneumonia, Cytomegalo viruses are the most accused agents in this sense(3). In ATP III guide published recently ,one of the criteria of metabolic syndrome and of the risk factors of CAD is enlarged waist circumference. In the case of the 23 year-old young paitent with MI, he has not Diabetes Mellitus, obesity (his BMI was 22.5kg/m² and his waist circumference 90cm) and his family didn’t have artery disease history.Also our case’s lipid profile wasn’t observed to be risky in comparision with pre-MI and HDL cholesterol (HDL: 61mg/dL) a positive risk factor was decreased. He wasn’t drug addicted, didn’t have a considerable stress factor and had an active life style. In our patient we researched newly-accepted risk factors as well as conventional, known parameters. His homocystein level was in a normal range. Lp (a) level was normal. CRP levels were in a range which wasn’t risky. In terms of insulin resistance, becoming popular risk factor after the detailed definiton of metabolic syndrome, the patient’s fasting insulin level was normal(8). Furthermore, the level of PAI-1 was in normal range and serologies of infectious agents were negative. In terms of factor V with Leiden mutation known to cause hypercoagulability and consequently increasing the risk of MI, the patient was found to be normal (3). The new parameters we found in our patient are seen in Table. The patient was researched in terms of vasculities ,as it is both a risk factor of CAD and likely to cause coronary disease which is not atherosclerotic, and it was excluded. When the level of the physical activity asked the patient who was a farmer declared regular sportive activity. It is known that social and psychological factors have important role in CAD as well. The patient’s social status and economic level was not risky.We were of the opinion that he had a cheerful and social character. The risk of CAD in young smokers is higher than that in non-smokers of the same age group (8). The risk of CAD in smokers has been shown to be directly proportional to the amount of smoking (9). 76%-91% of the young patients with MI are smokers (2). The fact that the patient in question was young, that he had smoked 30 cigarettes a day since he was ten ,that he didn’t have both conventional and newly-researched risk factors,have made us think strongly that smoking must have caused MI. Our aim in presenting this case was to show that in spite of high HDL cholesterol, smoking alone by itself can cause MI and to emphasize the importance of quitting smoking in earlier ages as it is recommended in mid and further age groups. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04023f2.jpg] [gm04023f1.jpg] [gm04023t1.jpg] [gm04023f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}