 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 3, 2004, pp. 16-20 ORIGINAL ARTICLE THE EFFECT OF SYSTEMIC VANCOMYCIN ON CENTRAL VENOUS CATHETER COLONIZATION Serkan Öncü1, Serhan Sakarya1, Pınar Okyay2, Ayşe Yıldırım3, Semra Çalangu4 Adnan Menderes University, Faculty of Medicine, Departments of Infectious Diseases-Clinical
Microbiology1 and Public Health2 Istanbul
University, Istanbul Faculty of Medicine, Departments of Anesthesiology3 and
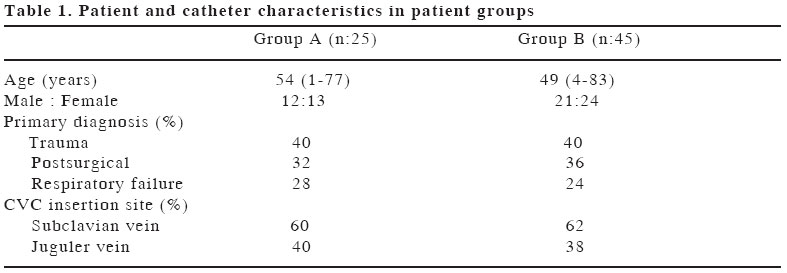
Infectious Diseases-Clinical Microbiology4 Code Number: gm04026 Central venous catheter (CVC) related infections are a major cause of morbidity and mortality. We undertook a clinical follow-up study in order to determine the value of systemic vancomycin usage before catheter insertion against catheter colonization. During the study period 70 patients with central venous catheters were prospectively studied. Patients were selected to one of two groups. All patients using vancomycin, without any other antibiotics, due to previous catheter related bacteraemia, were selected for group A. At the end of the vancomycin therapy a new CVC was inserted to a new site within an hour after the last dose (8 mg/kg). All the patients who had not used any antibiotics before and during catheter insertion were selected for Group B. None of the patients in both groups received any antibiotics for the duration that their catheters were kept in place. The catheters were removed at the end of the 7th day and cultured. In group A and group B colonization was detected with six (24.4%) and with 34 (75.6 %) CVCs, respectively. In group B colonization was detected with a significantly higher rate in comparison with group A with an odds ratio of 17.53 (95% CI: 4.150-7.054). In group A Gram positive cocci was not isolated from the catheter tip in comparison with group B in which the most commonly isolated organisms were Gram-positive cocci (n=21, 58.3%) (p<0.001). These results observed in a relatively homogeneous patient population, suggest that systemic usage of vancomycin before catheter insertion may reduce the incidence of CVC colonization, especially with Gram-positive cocci, and Gram-negative organisms dominate for the colonization. Keywords: Central venous catheter, vancomycin, colonization INTRODUCTION Central venous catheters (CVCs) have become essential tools for the management of patients in modern medical practice (1). They are used for the administration of intravenous fluids, medications, blood products, parenteral nutrition fluids, to provide haemodialysis, and to monitor the hemodynamic status of patients (2,3). Estimates of their use in the United States alone suggest that over 5 million CVCs are inserted annually (4). Unfortunately, these devices are associated with a number of complications, amongst which infection predominates (5). There has been a steady rise in the incidence of catheter -related infections (CRIs) despite emerging evidence-based measures to reduce infectious complications (4). More than 200,000 nosocomial bloodstream infections occur each year in the United States; most of these infections are related to different types of intravascular devices-in particular, the nontunneled CVC (5). Colonization of the catheter by microorganism is a critical step in the development of CRI (6,7). Most of the micro organisms implicated in catheter colonization and CRIs arise from the skin flora and Gram-positive cocci are responsible for most of the infections (8,9). We undertook a clinical follow-up study in order to determine the value of systemic vancomycin on catheter colonization especially with Gram-positive cocci. MATERIAL AND METHOD
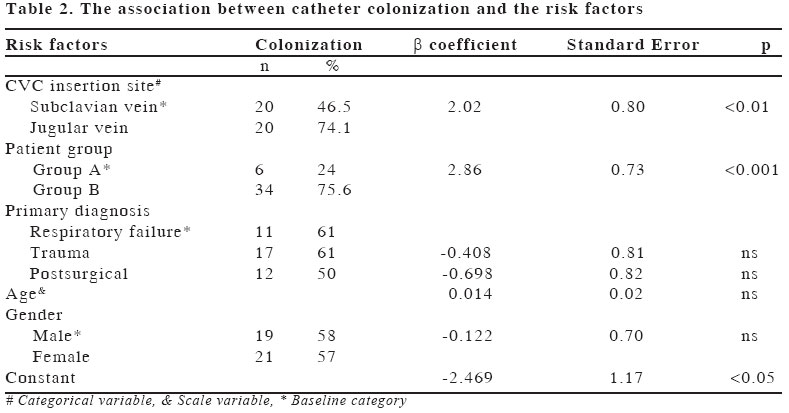
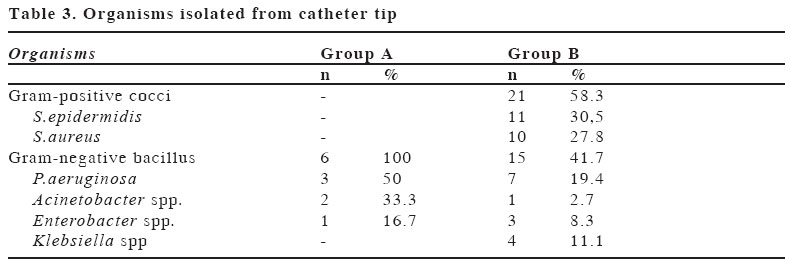
Our study was a clinical follow -up study conducted in Istanbul Medical Faculty and Adnan Menderes Medical Faculty. Patients admitted to ICUs between January 2002 and September 2002 who submitted to CVCs were clinically followed. Patients were included in group A or B, in accordance to following criteria. Group A Group B The catheters used were nontunneled, noncuffed, triple lumen and made of polyurethane material (Arrow, Erding, Germany). All catheters were inserted percutaneously using Seldinger technique in intensive care units (ICUs) under strict aseptic techniques by experienced anaesthetists. After washing hands and forearms with antiseptic soap, drying with a sterile towel, maximal sterile barrier precautions (sterile gloves, longsleeved sterile gown, mask, cap, and large sterile sheet drape) were observed prior to catheter insertion. Povidone-iodine was used as antiseptic for cleansing the CVC insertion site. After catheter insertion the site was covered with sterile gauze. Every 48 hours the dressing was removed, the site was inspected and cleansed with povidone-iodine, and a new dressing was applied. The catheters were removed at the end of the 7th day as scheduled replacement is followed in our hospital units. Each CVC was withdrawn aseptically using sterile forceps after the area of insertion was washed with povidone –iodine solution. The distal 5 cm of the catheter was cut off using sterile scissors and sent aseptically to the microbiology laboratory where it was cultured by semiquantitative method (10). Data were also obtained on patient age, gender, primary diagnosis on admission (categorized as trauma, postsurgical and respiratory failure) and CVC insertion site. Definition Statistical Method The logistic regression was used for risk assessment. Risk was given as Odds Ratio (OR) with 95% Confidence Intervals (CI). RESULTS A total of 70 patients were assessed in the study. The patients studied were 37 (52.9%) females and 33 (47.1%) males. The median age was 51.5 (1-83). The primary diagnosis of the patients were as follows; 28 (%40) trauma, 24 (34.3%) postsurgical, 18 (25.7%) respiratory failure. CVCs were inserted either into the subclavian vein (n:43, 61.4%) or into jugular vein (n:27, 38.6%). While 25 (35.7%) patients had received vancomycin before catheter insertion (group A), the other 45 (64.3%) patients were not using any antibiotics at the time of catheter insertion (group B). The patient and catheter characteristics of both group A and group B are presented in Table 1. Fourty (57.1%) of the CVCs were colonized. No significant differences were found for age, gender, primary diagnosis. Colonization was diagnosed with higher rate (n:20, 74.1%) in CVCs inserted via jugular vein in comparison with subclavian vein (n=20, 46.5%). The incidence of colonization was also higher in group B (n: 34, 75.6%) than in group A (n:6, 24%). Use of a jugular insertion site had an odds ratio of 7.531 (95% CI:1.570–6.119) compared with patients with a CVC inserted into the subclavian vein. When the patients using vancomycin before catheter insertion (group A) were taken as the reference category, the patients who were not using any antibiotics during catheterization (group B) had an increased risk with an odds ratio of 17.53 (95% CI: 4.15-7.05). The association between catheter colonization and the risk factors were given in Table 2. In group A, Gram-positive cocci was not isolated from catheter tip in contrast to group B in which most of the organisms isolated from the catheter tip was Gram-positive cocci (n:21,58.3%) (p<0.001). In group A the most commonly isolated organism from the catheter tip was Pseudomonas aeruginosa (n:3, 50%) followed by Acinetobacter spp (n: 2, 33.3%) and Enterobacter sp (n:1, 16.7%). In group B, S.epidermidis (n:11, 30.5%) was the most frequently isolated organism followed by S.aureus (n:10, 27.7%), P.aeruginosa (n:7, 19.4%), Klebsiella spp. (n:4, 11.1%), Enterobacter spp. (n:3, 8.3%) and Acinetobacter sp. (n:1, 2.7%) (Table 3). DISCUSSION CRIs are associated with increased mortality, morbidity, length of hospital stay and medical cost(2, 11). Infection rates vary greatly, depending on the type of device, and are highest with CVCs of all types (5). Many different risk factors for CRI in intensive care patients have been reported in the literature(9,12). These include insertion site, duration of catheterization, type of dressing, type of catheter, frequent manipulations, improper aseptic techniques, number of catheter lumens and type of topical antiseptic solution used. The only certain way of avoiding CRI is to avoid central venous access. The need for a CVC should always be considered on an individual patient basis. The catheter should also be removed as soon as practicable, as one of the most effective and cost -efficient way of reducing the incidence of CRI. Colonization of the catheter by microorganism is the first and critical step in the development of CRI (6, 7). Migration of skin organisms at the insertion site into the cutaneus catheter tract with colonization of the catheter tip is the most common route of infection for short-term catheters(10,13). We performed a study to assess the effect of systemic vancomycin usage on CVCs and found that the usage of vancomycin before catheter insertion was an independent factor which reduced catheter colonization especially with Gram positive cocci. The rate of colonization was 24% in group A in comparison with patients in group B in which the colonization rate was 76%. In the multivariate analysis, the CVCs inserted to patients in group B were associated with approximately 17 times increased risk of colonization compared with CVC inserted to patients in group A. These results observed in a relatively homogeneous patient population, considers that systemic usage of vancomycin before catheter insertion reduces the incidence of CVC colonization in patients needing CVC. The colonization rates in our study are higher than the most reported studies. The high rate of colonization especially for group B may reflect the fact that these patients were not on any antibiotics, unlike many other studies in which antibiotic usage were not taken for consideration. Gram-positive cocci are responsible for at least two-thirds of the CRI (8). Staphylococci are the most frequently isolated pathogens in CRI, particularly coagulase-negative Staphylococci (CNS) followed by S.aureus and enterococci (14). In group A, Gram-positive cocci was not isolated from catheter tip in contrast to group B in which most of the isolated organisms were Gram positive cocci. Vancomycin is a glycopeptide antibiotic active against Gram –positive organisms and it seems that it’s systemic usage before catheter insertion prevent colonization of CVCs. As colonization is accepted as an essential step in the pathogenesis of CRI, the systemic usage of vancomycin should also prevent CRI (7). But scientific studies on the efficacy of this practice are inconclusive. In four published studies of systematically administered antimicrobials it was suggested that antimicrobials administered at the time of or immediately after insertion of a CVC may reduce the incidence of CRI (1,9,15-17). Other trials demonstrated no benefit of such prophylaxis (18-20). But these studies did not take the antibiotic usage after catheter insertion into consideration. So, our study is the first study in which the patients had not used any antibiotics after CVC insertion. We think that antibiotic usage after catheter insertion may affect the colonization rate and the causative agent of the colonization. Most studies have found a high level of concordance between microorganisms found on the skin at the insertion site and organisms subsequently found on the catheter tip (13, 21, 22). Bacteria may contaminate the catheter tip at the time of insertion and subsequently cause CRI (7). Our study supports their conclusion; giving an antibiotic effective against Gram –positive cocci reduce the CVC colonization with these organisms. Empiric treatment, when indicated, should provide coverage against the most frequent organisms causing CRI. Even though local epidemiology must be taken into account, certain organisms should always be considered. Gram-positive cocci are the leading cause of CRI according to all studies, being responsible for more than 60% of episodes. As reported in our previous study (9), this study also considers that CRI in patients whose CVC was inserted during the therapy with antibiotics effective against Gram -positive cocci, Gram -negative organisms should also be suspected as the cause of CRI and antibiotics which are also effective against these pathogens should be started empirically. Use of systemic vancomycin is associated with development of intermediate resistance to vancomycin and subpopulations of Gram-positive cocci with reduced vancomycin susceptibility (23-25). Therefore systemic usage of vancomycin should strictly be avoided for the prevention of CRI. Efforts should be focused on interventions that are not likely to encourage the emergence of antimicrobial resistance, such as maximal barrier precautions. In summary, these results, observed in a relatively homogeneous patient population, suggests that systemic usage of vancomycin may reduce the incidence of colonization in CVCs, especially with Gram-positive cocci. But further prospective, randomized clinical studies are needed to evaluate the effect of systemic antibiotic usage on catheter colonization and also on CRI. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04026t2.jpg] [gm04026t3.jpg] [gm04026t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}