 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 3, 2004, pp. 21-25 ORIGINAL ARTICLE ENURESIS NOCTURNA PREVALENCE AND RISK FACTORS AMONG SCHOOL AGE CHILDREN IN NORTHWEST TURKEY Murat Unalacak1, Ayhan Söğüt2, Erol Aktunç1, Nejat Demircan1, Remzi Altın3 Zonguldak Karaelmas University, Faculty of Medicine, Departments of 1Family
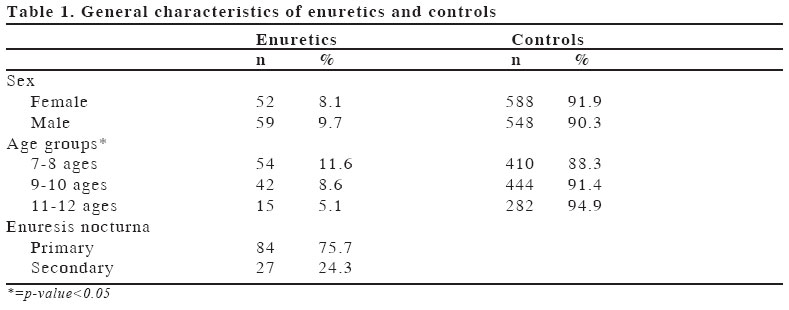
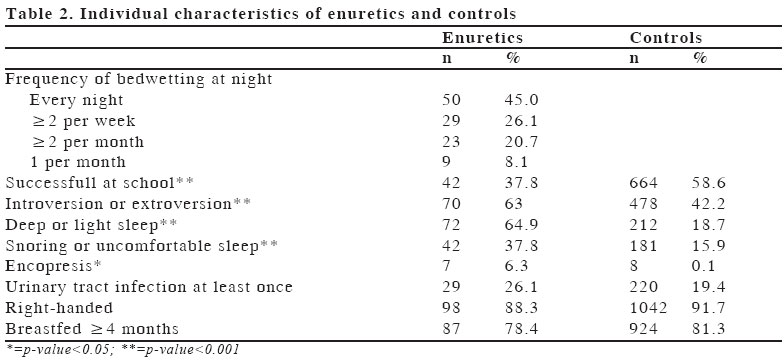
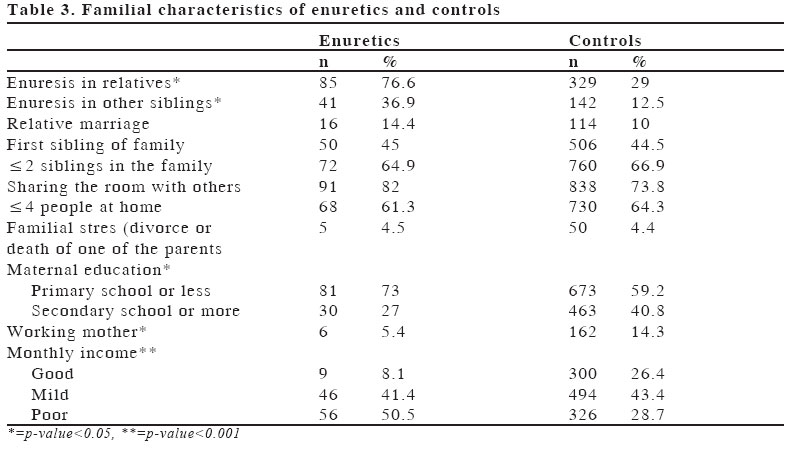
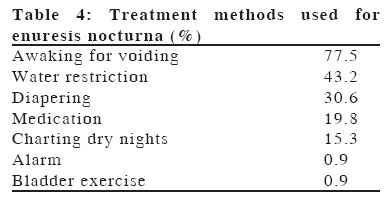
Medicine, 2Paediatrics and 3Pulmonary Medicine Code Number: gm04027 To find out prevalence of enuresis nocturna (EN) among school age children, and to determine associated factors and regional differences, an epidemiological study was performed among children between 7 to 12 years living in Zonguldak, Turkey. Data were collected at schools by a questionnaire. EN prevalence was found as 8.9 %, most (75.7 %) were primary, and the rest were secondary. Prevalence decreased as the age increased in both genders. There was a positive relationship of EN with positive family history, presence of EN in a brother or a sister, encopresis, sleep disturbances, a maternal education of primary school or less, working mother, low monthly income, low school success and introversion or extroversion. Only 19.8 % of the cases preferred medical treatment modalities, other preferences were waiting for spontaneous improvement, awaking the child for voiding, water restriction and diapering, in decreasing order. As EN is a disease that can result in low self-esteem, some other psychological problems and low school success, it must be treated. Informing these parents wherever they are met, especially at primary health care settings, is necessary both not to miss patients and to convince the parents for treatment. Key words: Enuresis nocturna, risk factors, children, Turkey INTRODUCTION Enuresis nocturna (EN) is a common health problem all over the world [1, 2, 3]. This disease, although seems to be ordinary, is crucial to be diagnosed and treated as soon as possible, as it can result in some psychological consequences, such as low self-esteem [4]. But usually parents prefer to wait for self-recovery, or to use traditional methods, as the disease is considered to be harmless and self-limited [5, 6]. It has already been known that EN is not of great concern in Turkish families [7]. Many etiological factors are mentioned for EN, but it is an impeding factor against efforts on treatment modalities that there is no consensus of opinion about its aetiology. Offered time for toilet training is after 2 years of age. This corresponds to the time when sphincter and spinal reflex coordination starts to mature. This process is completed generally at the age of four [8, 9]. Only a few studies were conducted in Turkey about prevalence of EN, and these were carried on in southwest regions. We planned this study to determine prevalence of EN and associated factors among children between 7-12 ages and to see whether there were regional and climatic differences. Also some factors that could be associated with enuresis and that had been investigated in southwest of Turkey in previous studies were also interrogated in our study, and evaluation was made by taking climatic factors into consideration. For this purpose, a questionnaire including questions about presence or absence, and characteristics of EN and some socio-economic and cultural factors, was established, and prevalence of EN among children between 7-12 ages and co-variance with somatic, behavioural and socio-cultural factors were investigated. MATERIAL AND METHODS Zonguldak is a mountainous city located in the northwest of Turkey, with a population of about 106000. A sample of 1350 students, representative for the primary school population of Zonguldak, were included in the study; all were between 7-12 ages and from 12 schools located in different regions of the city. A special questionnaire was preparedabout demographic, socio-economical, familial and physical status of the children, whether he or she had EN, encopresis, frequency of EN, familial history, treatment modalities, and distributed to the randomly selected students in these schools, and the parents of the students were requested to complete the questionnaire. Questionnaires were distributed and collected within sealed envelopes in order to prevent embarrassment of the children. Parents were informed about the study by an information section included in the questionnaire. Of the 1350 questionnaires distributed, 1288 (95.4 %) were collected, and of these, 1247 (92.4 %) that were eligible were evaluated. Seventy-two percent of the questionnaires were completed by the mother, 19% by the father, and the remaining 9% by other relatives. EN was defined as unaware bedwetting at night at least once a month after 5 years of age. Primary enuresis was defined as bedwetting at least once a week who had never had nighttime bladder control for 6 months or more. Secondary enuresis was considered when the child has been toilet trained for at least six months after the age of bladder control, and the bladder control has been subsequently lost (10) Encopresis was defined as passage of feces into inappropriate places after chronological age of 4 years (11). The children having EN were taken as cases, and the others as controls. Statistical analyses were done by chi-square test. All analyses were performed with SPSS for Windows, release 11. This study has been approved by City Educational Office in Zonguldak. RESULTS Of the subjects, 48.7 % were males and 51.3 % were females. Mean age of the subjects was 9.17 (SD: 1.47) years. Among analysed children, 111 (8.9 %) had EN. Of the enuretic patients, 53.2 % were males and 46.8 % were females, and EN was found in 9.7 % of males and 8.1 % of females. No gender predominance was observed. Of the cases, 24.3 % had secondary EN, and 75.7 % had primary EN. Most of the cases were observed before or at 8 years of age (Table 1), while only 0.3 % occurred at the age of 12 (p<0.05). In 45 % of the cases, bed-wetting occurred every night (Table 2), and an average of 3.95 wet nights occurred weekly due to enuresis. Average of bed-wettings per night was 1.5. Sleep disturbances such as deep sleep or light sleep, snoring or lack of a comfortable sleep, and psychological problems such as introversion or extroversion, low school success, were encountered more frequently among enuretics. Also encopresis was encountered more among enuretics (Table 2). EN history in relatives, history in a brother or a sister alone, a maternal education of primary school or less, housewife mothers, familial stress (divorce, or death of one or both of the parents), low monthly income, were encountered more frequently among enuretic children (Table 3). Urinary tract infection at least once in lifetime did not differ significantly between enuretics and controls (Table 2). Marriage with a relative, being the first sibling of the family, being breastfed or not at least for four months, total number of siblings, being left-or right-handed, number of family members living in the same dwelling, number of family members sleeping in the same room with the enuretic child were not found to be related with frequency of EN (Tables 2 and 3). Only 22 (19.8 %) of the cases used medication for treatment of the disease. Desmopressin and imipramin were the most commonly (86.4 %) prescribed drugs. The other methods used in treatment of EN shown in Table 4. DISCUSSIONEN is a common health problem among Turkish children, as in many other populations [1, 2, 3, 7, 12]. This is a population-based study, which aimed to detect prevalence and risk factors of EN in Zonguldak, a city in northwest of Turkey. A high response rate (95.4 %) was achieved, probably due to the distribution method of the questionnaires, that is, by the way of teachers, and it might be perceived as an assignment. Prevalence of EN was found 8.9 %, and this was less than 11.5 % reported by Serel et al. [1] in Isparta, 13.7 % reported by Gümüş et al. [12] in Manisa and 11.6 % reported by Öge et al. [7] in Aydın. This difference might be due to sociocultural variations and attitude and behavioral differences of the parents between the regions. All these cities are located in southwest of Turkey, under the influence of Mediterranean climate, which differ from rainy climate of Zonguldak. Humidity is higher in Zonguldak, as it is a seaside city, and it gets much more rain than the southwestern cities of Turkey. Also the temperature is usually 3-5oC lower in Zonguldak than the southwestern cities. So we speculate that climatic changes might affect EN prevalence, as mentioned by Cederblad et al. [13]. EN prevalence was found between 5.5 % and 56.4 % in other countries [7, 13-19]. No gender predominance was observed for EN, although male predominance was detected in some other studies performed in Turkey [1, 7], and in some performed in other countries [14, 16]. As found in other studies [1, 14, 18], number of enuretics decreased as the age increased. As EN is mostly expected to improve spontaneously, decrease with age is thought to be mostly due to spontaneous improvement. Besides other factors, role of heredity was found to be important in aetiology of EN in previous studies [7, 20]. In our study, consistent with the literature, EN was found to be more in children with positive family history. History in a brother or a sister was also significantly increased. As the disease is mostly found in the childhood period of the parents or in other siblings or the relatives, they take it to be familial. Also as there is a widespread belief that drugs used in EN cause impotence, most families are reluctant to use them for such a condition mostly believed to be harmless. Gümüş et al. established a higher EN prevalence with lower parental education level [12]. However, Tsang-Wee et al. showed a greater prevalence rate in children with parents of a higher educational status [14]. Öge et al. and Hanafin et al. found that low socio-economic status was a significant factor related with enuresis [7, 20]. In our study, both a maternal education of primary school or less and low monthly income as a representative of economical problems were found to be related with an increased prevalence of EN. A maternal education of primary school or less is also thought to form a base for formation of wrong beliefs about medications. Working mothers were found to have less enuretic children than housewives. This was thought to be due to higher education level of working mothers in our region. Encopresis was found to be more among enuretic children. This is consistent with the previous literature [16, 21]. This may be caused by same socio-economical conditions or other etiological factors resulting in EN. Cederblad et al. found that pre-school enuretics and two thirds of the school age enuretics used to sleep very heavily [13]. Kalo et al. and Rosenfeld et al. found that deep sleep was significantly more among enuretic children compared with non-enuretics [16, 22]. In our study, we found a positive correlation of heavy sleep, light sleep, snoring and lack of a comfortable sleep with EN. School success of enuretic children was found to be significantly lower than that of controls. Also introversion or extroversion was more frequently faced in EN cases. These can be related with attitude and behaviour of the family and other people to the enuretic child. Also psychological problems can result in low school success, which is frequently observed in enuretics in our study. Only 22 (19.8 %) of the cases used medication for treatment of the disease, partially due to mentioned traditional beliefs. Usually parents prefer to wait for self-recovery, or use traditional methods, as EN is not considered as a condition to be treated among Turkish families [7]. In our study, most commonly used methods for treatment were awaking the child for voiding, water restriction and diapering, in decreasing order (Table 4). As a conclusion, EN must be treated, as it is a disease that can result in low self-esteem, some secondary psychological problems, and low school success. It is necessary to inform the parents wherever they are met, especially at primary health care settings. For this purpose, health educators and primary care health staff must be educated for eliciting a detailed history not to miss patients. Explaining detrimental effects of EN and presenting true information about the medications are important for convincing the parents for treatment. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04027t4.jpg] [gm04027t3.jpg] [gm04027t2.jpg] [gm04027t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}