 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
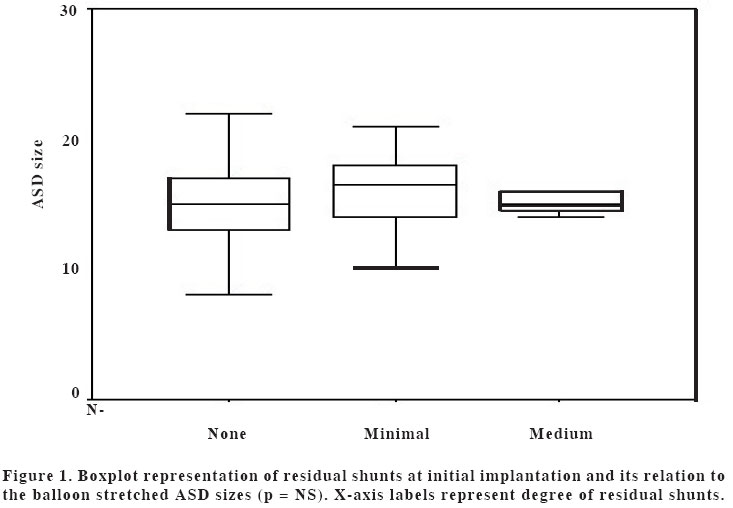
European Journal of General Medicine, Vol. 1, No. 3, 2004, pp. 33-36 ORIGINAL ARTICLE TRANSCATHETER CLOSURE OF ATRIAL SEPTAL DEFECTS: EXPERIENCE OF A PEDIATRIC HEART CENTER Volkan Tuzcu, Ina Michel-Behnke, Dietmar Schranz Children`s Heart Center, Justus-Liebig University Giessen Code Number: gm04029 Transcatheter closure of the ASDs has become the procedure of choice for most centers. In this article, we report our experience in 129 children who have undergone transcatheter closure of their ASDs. The balloon stretched diameter of the ASDs ranged between 6 and 28 mm. The immediate success rate for device closure was 92% and closure success rate was 98% at one year follow-up. There was no significant relationship between the ASD size and the initial-implant success rate (p =NS). Multifenestrated ASDs were present in 18% of patients. Significant complications, including device embolization, aortic root erosion, thrombus formation, and 1st degree AV block, occurred in 6% of patients. There were no procedure related deaths, and there were no residual adverse effects in patients who required removal of their devices. Transcatheter device closure of ASDs is an effective and safe procedure with elimination of intraatrial shunts in vast majority of patients, and this should be the procedure of choice for the closure of ASDs which are amenable to device closure. Key words: ASD, transcatheter closure INTRODUCTION Transcatheter closure of ASDs has become the procedure of choice for treatment of ASDs in many centers (1,2). High success rate, low complication rate, and ease of application are the main advantages of this approach. In this article, we report our experience of transcatheter device closure in children. There have been significant developments over time which resulted in devices with better outcomes. Initial attempts for transcatheter device closures were associated with higher complication rates compared to today (3). This problem was overcome overtime with the better designs of the devices. A retrievable device, Amplatzer septal occluder (AGA Medical Corporation, Golden Valley, Minnesota, USA) became the device of choice for most interventional cardiologists (4,5). In this article, we report our experience in 129 consecutive transcatheter ASD closures between September 1996 and December 2002. We also report our intermediate term follow-up results. MATERIAL AND METHODS Study Population Statistical Analysis RESULTS Total of 85 Amplatzer, 20 Angelwing, 10 Cardioseal, 10 Starflex, and 4 Helex devices were implanted during that period. Average procedure time was 111.7 + 49 minutes. Average fluoroscopy time was 9.6 +7.4 minutes. Device selection was per operator`s preference, however after September 1999, predominantly preferred device was Amplatzer (90% of devices between September 1999 and December 2002). Mean native diameter of the ASDs with transthoracic echocardiogram measurements was 10.6 + 3.5 mm (4 to 25 mm), and mean balloon stretched diameter of the ASDs was 15.6 + 3.5 mm (6 to 28 mm). Initial closure success rate was 92% (No residual shunts in 90 and minimal shunts in 29 cases). Medium amount of shunts were present in 8 patients. Average follow-up was 926 + 592 days. Follow-up data was available in 95 patients at 1 year. At 1 year closure success rate was 98%. Two patients continued to have medium amount and 2 patients had minimal amount of residual shunts. Rest of the patients did not have any residual shunts. At 2 year follow-up, other then the 2 patients with medium amount shunts, no other shunts were observed. Both of these patients had multifenestrated ASDs and both patients required removal of the devices, one surgically, other by interventional approach. Overall success rate was 97% (65 of 67 patients) at 2 years. The comparison of the various type of ASD devices revealed some differences. Immediate closure success rates were as follows: Amplatzer device: % 96 (82 of 85), Cardioseal: 60% (6 of 10), Angelwing: 100% (20 of 20), Helex: 100% (4 of 4), and Starflex: 90% (9 of 10). At one year follow-up: Amplatzer device: 100% (57 of 57), Cardioseal: 78% (7 of 9), Angelwing: 100% (20 of 20), Helex (no follow-up available), and Starflex: 100% (10 of 10). At the initial implantation time 4 of 10 Cardioseal cases had medium amount of shunts. One of these patients had decreasing shunt over time and at 2 year follow-up there was no residual shunt. Two of these patients continued to have medium amount of shunts at 2 year follow-up. Both of these patients had multifenestrated ASDs and because of significant persistent residual shunts they both had surgical closure of their residual ASDs. In one patient with medium amount of shunt in that group, no follow-up data was available after implantation. One-way ANOVA did not show any significant relationship between the ASD size and the initial-implant success rate (p = NS) (Figure 1). We were able to close ASDs up to 28 mm in diameter successfully. Among the 129 cases, single ASDs were present in 106 and multifenestrated ASDs were present in 23 patients. Closure success rate was 96% (102 of 106 patients) in single ASDs and 82% (19 of 23 patients) in multifenestrated ASDs. This difference was statistically significant (p < 0.05). Procedure-related complications were as follows: 3 devices embolized, one was removed surgically and rest of them were removed with interventional approach using snare catheters. One patient had erosion of the aortic root with effusion. This required surgical removal of the device. One patient developed 1st degree AV block. One device was not in acceptable position and had to be surgically removed. Two patients had evidence of thrombi. One had suspected thrombus in the pulmonary arteries, and in the other one thrombus was located on the left atrial disk of the ASD device. There were no procedure related deaths, and there were no residual adverse effects in patients who required removal of their devices. DISCUSSION This report shows that transcatheter closure of the ASDs can be safely performed in children with a high success rate. Amplatzer device seems to be very effective and easily applicable with probably less complications compared to other device models (7,8). Even large ASDs can be closed with Amplatzer device successfully unlike other devices (9). Although we reported the comparison of different ASD devices, there was not enough number of cases to make that comparison statistically significant. The fact that Amplatzer device can easily be repositioned or retrieved in the event of an unacceptable position, contributes to the high success rate and the low complication rate (5). This device became the device of choice for most centers utilizing this technique. In many centers, surgical closure of ASDs is only considered when ASD is not appropriate for transcatheter closure (10). Our results are also supportive of the high success rates for Amplatzer device closure of ASDs in children. Our experience revealed a high success rate for transcatheter closure of ASDs with very low complication rate at the intermediate-term follow-up. Two patients had significant complications. One patient had aortic root erosion which occurred 3 months following implantation. This patient had an Angelwing device and was noted to have pericardial effusion on echocardiogram at 3 month follow-up. The device was explanted and the defect was repaired surgically. Another patient had thrombus formation on the left atrial disc of 26-mm Amplatzer device. Of note, majority of the initial shunts were minimal shunts and at 2 year follow-up there was no patient with residual minimal shunts. The ASD-closure success rates were very similar between the 1st year and 2nd year follow-up visits (% 98 and % 97). The higher success rate at these follow-up visits was due to the decrease of shunts in some patients who initially had medium amount of shunts. In conclusion, transcatheter closure of ASDs can be safely and effectively performed in children. Elimination of intraatrial shunt can be achieved in 97% of the patients. Even the multifenestrated ASDs can be closed successfully with this technique. The intermediate follow-up results are very encouraging and this should be the procedure of choice for the ASDs who are amenable to transcatheter closure. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04029f1.jpg] |
| |||||||||

{kind=link}