 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 3, 2004, pp. 45-48 CASE REPORT VASCULAR PATHOLOGY OF THE GREATER OMENTUM: Report of two cases Montiel-Jarquin A.J1, Sanabria-Macias2, Sanchez-Turati J.G1, Iturbide-Garcia J2, Sandoval-Cruz M.V.H3, Ramos-Alvarez G4 Hospital General Regional, “San Alejandro”Instituto Mexicano Del
Seguro Social, Departments of General and Laparoscopic Surgery1,
Pregrade Internship Student2, Radiology3 ,
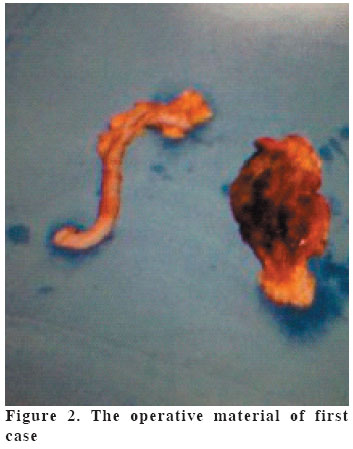
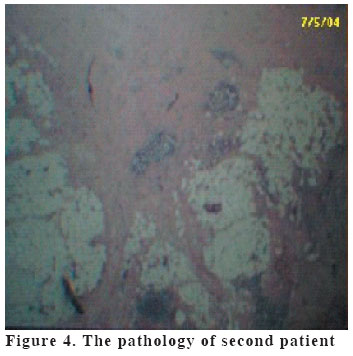
and Pediatry4 Code Number: gm04032 Vascular pathology of the greater omentum is still being very rare, since Bush described the first case in 1896. The objectives are to describe two clinical cases, the first one about right-sided segmental torsion of the greater omentum and the other one about infarction of the greater omentum, which were diagnosed and treated in our hospital; as well as to check pertinent literature. In first case, a forty year old male, thin, with one week evolution: right lower quadrant pain, nausea, hiporexia, a previous prescription of an antiamebic and antispasmodic with no healing, fever, mild leukocytosis, neutrophilia, Simple X ray of the abdomen suggesting acute appendicitis. The patient underwent Exploratory Laparotomy which revealed right-sided segmental torsion of the greater omentum. In second case, a thirty year old female, thin, presenting a six day evolution: pain in the whole right hemiabdomen, difficulty for walking, abdominal distention, hiporexia, fever, bad general condition, with a previous prescription based on metamizol, ampicilin with no healing, mild leukocytosis, neutrophilia and simple X-ray of the abdomen also suggesting acute appendicitis. This patient was also surgically treated with the diagnosis of right-sided segmental infarction of the greater omentum. In conclusion, vascular pathology of the Greater Omentum is still being very rare. Its clinical presentation is nonspecific and forms a great part of pathology which causes right lower quadrant pain, commonly confused with acute appendicitis. Despite medical breakthrough its diagnosis is difficult. The treatment is surgical, evolution is good if the treatment is adequate, and prognosis is favorable. Key words: Infarction, right-sided segmental torsion, greater omentum. INTRODUCTION Surgical pathology of the greater omentum is very rare and includes torsion, infarction, cysts and solid tumors. The first case of right-sided segmental torsion of the greater omentum (RSSTGO) was described by Bush (1) in 1896 and by the year 1908 one hundred and twelve cases had been described; (2) In 1991 Coppo gathered about one hundred fifty cases (3). Helmrath in 2001 found over three hundred described cases of Infarction of the greater omentum (IGO) (4). Nowadays both pathologies can be considered as rare causes of Right Lower Quadrant Pain (RLQP) (5). About the 85% of the cases have been reported in adult population, remaining 15% in pediatric population (4). Due to its nonspecific symptomatology the preoperative diagnosis is often confused with acute appendicitis because it is the most frequent cause of abdominal pain (5,6,7,8). RSSTGO and IGO are rare pathologies included in a vast list of pathologies which cause chirurgical acute abdomen (9,10,11). The present paper describes two clinical cases of adult patients the first with RSSTGO and the second with IGO, its clinical condition, diagnosis, treatment and evolution as well as literature review. CASE 1 A twenty six years old, thin male, no relevant background who was committed to our hospital with a clinical history of one week evolution presenting nausea, hiporexia and RLQP. The patient was previously given metronidazole, butilhioscine with no healing. He arrived to the hospital: with 120/70 mmHg. blood pressure, 92 pulse rate, 20 respiratory rates, 38.1 Celsius degrees body temperature, no peritoneal irritation, RLQpain, and rebound tenderness. The white blood cell count was 11200/mm3, 84% neutrophils, plain film of the abdomen revealed scoliosis, undefined shape of the right-sided psoas muscle, ileus and undefined shape of the sacro iliac joint (Figure 1). With the presumptive diagnosis of acute appendicitis exploratory laparotomy was done which was revealed hemorrhage, fibrin and vascular infarction in an area of about ten square cms. due to RSSTGO (Figure 2). The affected area of the greater omentum was resected and also appendectomy was performed. CASE 2 A twenty year old female, patient, who came to our hospital without relevant gynecologic background, six days previous to the arrival she presented, RLQP, difficulty for walking, abdominal distension, hypoxia, fever and bad general condition. She was medicated with metamizole and ampiciline with no healing.Physical examination revealed 120/ 65 mmHg blood pressure, 99/min pulse rate, 18/min respiratory rate, 38.4, Celsius degrees body temperature, normal heart and lung findings, distended, diminished peristalsis sounds, RLQP and reboundtenderness. The lab tests showed 12200/mm3 leukocytes, 79% neutrophils; plain film of the abdomen showed scoliosis, persistent loop in the right lower quadrant and air-gas levels (Figure 3). The patient underwent surgery with a preoperatory diagnosis of acute appendicitis, but hemorrhage, necrosis and vascular infarction in the greater omentum (Figure 4). was revealed the affected area in the omentum was resected as long as appendectomy. In both patients it was not possible to establish the cause of the lesion. Both of them evolved in a satisfactory way and were discharged from the hospital after 3 days. DISCUSSION RSST and IOGO are still rare nosologyc entities up to now. Since 1896 when Bush described the first case, three hundred have been reported. (1) Both pathologies are recognized as a common cause of acute abdomen whose similarities with acute appendicitis, can occur at any age and its etiology remains uncertain. (7,12,13) Infarction and torsions of the greater omentum are considered as idiopathic entities. (12,13) Despite of its uncertain etiology, the predisposing factors are obesity, (14,15,16) sex, traumas, autonomics (large pedicle), violent exercise, accelerated peristalsis and adherences. Symptoms correspond to a whole acute abdomen frequently confused with acute appendicitis, gynecologic disorders among others. (17) The patients present right and left lower quadrant pain, right upper quadrant pain, depending on the location of the lesion; nausea, vomiting and diarrhea, constipation, fever, anorexia; white blood cell count can be normal or slightly elevated and a mass can be palpated at physical examination, rebound and acute appendicitis signs. The diagnosis can be supported by ultrasound which reveals a hiperecoic ovoid mass and more specifically by Computed Axial Tomography or Magnetic Resonance Image, that show more circumscribed lesions with interposed fat, hyper-attenuated areas generally localized in the right hemiabdomen; (4,7,15,18) laparoscopy can be diagnostic or curative. (5,19,20) Early operative intervention is necessary to avoid the increased morbidity and mortality associated with peritonitis. (21) During the laparotomic approach, if we do not find acute appendicitis and we find hemorrhagic liquid we should look for: ovarian torsion, bleeding Von Graff follicle; transparent liquid: intestinal occlusion; turbid liquid: bacterial or chemical peritonitis; fecaloide smell with turbid liquid: intestinal perforation; if we do not find liquid of peritoneal reaction: we should look for Meckel’s diverticulitis, Crohn’s disease, intestinal invagination; thinning of the terminal ileum and caecum: we should aspire the intestinal liquid to look for Salmonella, Shigella and Yersinia; when infarcted lymphatic nodes were found. We must take a biopsy for histopathological examination. If all this is apparently normal, we should enlarge the incision to look for pathology in the greater omentum and to continue exploring the rest of the abdominal cavity, pelvis and retro-peritoneum, proceeding to appendectomy before ending the surgical act or taking out the laparoscopic camera. (9,11,14,16) Torsions and infarctions of the greater omentum are still unusual pathologies. Treatment includes resection of the affected area of the greater omentum, resection of the cecal appendice and release of the adherences by means of Laparoscopy or exploratory laparotomy (14). As in literature, in our patients preoperatory diagnosis was acute appendicitis and with the resection of the affected segment of the greater omentum, evolution was good, getting into the cure. Evolution is good, curative in 100% of the cases; however a conservative treatment can be done when preoperatory diagnosis by ultrasound, computed axial tomography or magnetic resonance image is practiced. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04032f1.jpg] [gm04032f2.jpg] [gm04032f3.jpg] [gm04032f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}