 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
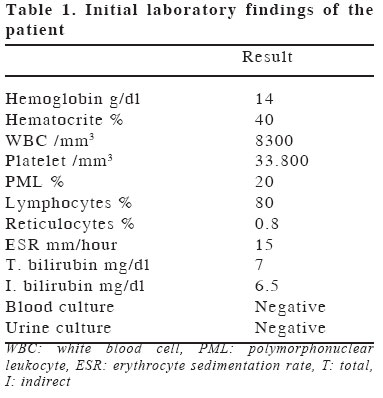
European Journal of General Medicine, Vol. 1, No. 3, 2004, pp. 49-50 CASE REPORT UNUSUAL PRESENTATION OF CONGENITAL PLASMODIUM VIVAX MALARIA IN A NEONATE FROM TURKEY Fuat Gürkan, Meki Bilici, Mehmet Davutoğlu, Heybet Tüzün, İclal A. Sucaklı Dicle University, Faculty of Medicine, Department of Pediatrics Code Number: gm04033 A 28-day-old full-term male neonate was admitted with symptoms and findings of jaundice, hepatosplenomegaly, thrombocytopenia and a cavernous hemangioma on the forearm. Patient’s mother gave a history of antimalarial drug usage before pregnancy. He did not have characteristic symptoms like fever and chills at presentation, and had an associated hemangioma which could partly explain the jaundice and thrombocytopenia. The diagnosis of congenital malaria was established only when Plasmodium vivax was detected after the third blood smear. Key words: Congenital malaria, Plasmodium vivax, diagnosis INTRODUCTION Most case reports on congenital malaria in Europe are imported cases from endemic areas outside of Europe, most of them being of Plasmodium falciparum (1,2). Here, I present my expierence of an unusual presentation of an authochthonous case with congenital Plasmodium vivax malaria in Diyarbakir, Turkey and discuss the early identification and management of the disease. CASE A 28-day-old full-term male neonate, born via normal vaginal delivery from a Turkish mother, was admitted to our clinics with symptoms of jaundice beginning from the third day of life and a cavernous hemangioma on the forearm. On admission, the infant was in well-apperance and vital signs were normal with a rectal temperature of 37.5oC. Growth percentiles were in normal ranges. On the physical examination, there were remarkable jaundice, scleral icterus and hepatosplenomegaly. The infant was afebrile throughout the hospital course. Initial laboratory findings are shown in the Table. Serology for hepatitis, toxoplasmosis, rubella, cytomegalovirus and herpes infections were negative. Thyroid hormones and metabolic screening were normal. In the third blood smear of our patient, P.vivax was detected; and thick smears were positive for malaria parasites with a low parasite density. Our patient’s mother and other five family members were asymptomatic and repeatedly tested negative on blood films for malaria parasites. The patient was treated with oral chloroquine phosphate, 10 mg/kg of base as an initial dose, followed by 5 mg/kg of base at 6, 24 and 48 hours. The patient was discharged without parasitemia after the third day of diagnosis. DISCUSSIONThrough concentrated efforts for malaria eradication programme in Turkey, number of recent malaria cases has changed according to years with a marked deterioration with 84.345 cases in 1994 and a steady decline to 20.963 cases in 1999 (3). Although our province is at an endemic region for malaria in Turkey, no previously reported case with congenital malaria has been detected. Congenital malaria is known as an uncommon disease even in endemic areas, since the transmission of malarial parasites from the mother to the fetus is uncommon due to the barrier action of placenta. (4). Another case with congenital malaria was reported in a non-endemic city in Turkey in 1999 (5). Our patient’s mother gave a history of antimalarial drug usage before pregnancy. Infants of mothers with chronic subclinical infections may be protected by maternal IgG (1,6,7). Asymtomatic cases of P.vivax do not have circulating erythrocytic stages and this makes the transmission to the fetus even more surprising. In most studies from isolated endemic areas in other countries, congenital malaria with P. falciparum was found to be predominating. Our patient had jaundice, hepatosplenomegaly and thrombocytopenia at presentation, but not fever and chills. A classic presentation of malaria may not occur at the newborn, since these parasites can only use reticulocytes for replication and these cells are scarce in newborns due to depressed erythropoesis after birth (8). In these situations it is more difficult to establish the diagnosis and a good index of suspicion, a careful physical examination and repeated peripheral blood smears are needed. Sometimes parasitemia cannot be shown on blood smear, and plasmodial antigen detection or polymerase chain reaction (PCR) of the blood may be necessary. The prolonged jaundice and thrombocytopenia were first thought to be due to cavernous hemangioma in our patient. In the treatment of our patient primarily chloroquine was used. Primaquin is not needed for the newborn infant, because no persistent liver phase exists in congenitally acquired infections, and it can cause methaemoglobinemia which can be fatal at that age. Our patient’s mother did not take any medication during pregnancy, but chloroquine therapy is recommended for the pregnant women prophylactically once weekly until after delivery (4,5). Re-infections or treatment failures have been reported to be common (6). Congenital malaria is known to result in abortion, prematurity, low birth weight and neonatal death (1,5), but there is no knowledge that malformation can be caused by plasmodia. The co-existence of cavernous hemangioma as a congenital malformation in our patient with congenital malaria seems to be coincidental, but an in-utero causal relationship can be debated if supported by other similar cases. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04033t1.jpg] |
| |||||||||

{kind=link}