 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 3, 2004, pp. 51-54 CASE REPORT SPONTANEOUS RUPTURE OF THE SPLEEN IN A HEMODIALYSIS PATIENT Mustafa Aldemir1, Ali Süner2, Veysel Kıdır2, Ozan Balakan2, Tahir Çelenk2 Dicle University, Faculty of Medicine, Departments of General Surgery1 and
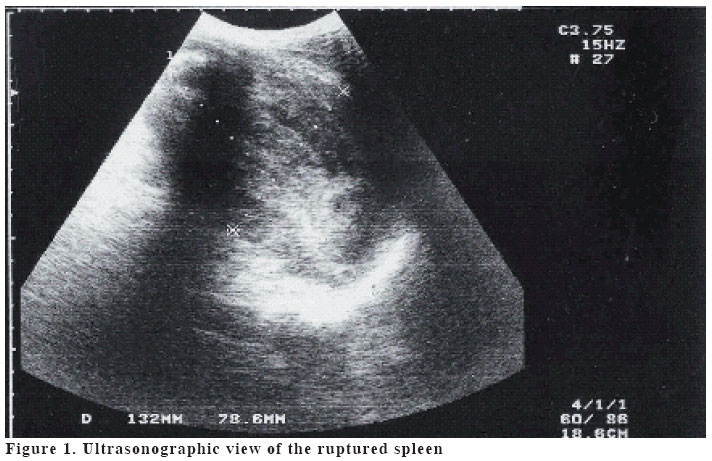
Internal medicine2 Code Number: gm04034 Hypovolemic shock and spontaneous splenic rupture (SSR) are unusual fatal complications in the uraemic patients. We described a case of SSR in a 29-year-old hemodialysis (HD) patient. The diagnosis was confirmed with the acute abdomen picture included the left upper abdominal and left shoulder pain together with shock and ultrasound findings. The splenectomy was performed. The postoperative course was uneventful and the patient was discharged from hospital on the 5th day. The mechanism of the rupture is still unknown, but the rupture and subcapsular haematomas of spleen may be induced by the uraemic coagulopathy, the use of anticoagulants during HD, malignant hypertension and unrecognised microtrauma. Splenic rupture should be considered in any patient with abdominal pain and shock, regardless of a history of trauma or previously known risk factors for spontaneous rupture. An aggressive multidisciplinary approach to the management of these patients may decrease the mortality rate. Key words: Spleen rupture, hemodialysis. INTRODUCTION Spontaneous splenic rupture (SSR) is an uncommon but important clinical entity. Unfortunately, the diagnosis is often missed due to the absence of any history of trauma (1). The SSR has been unusually shown inpatients with end-stage renal disease treated with hemodialysis (HD) (2-4) and continuous ambulatory peritoneal dialysis (CAPD) (5,6). This severe complication may be related to splenic infarction due to conditions such as atherosclerosis, diabetes mellitus, polycytemia, amyloidosis (2,5,7,8) uremic coagulopathy and the use of heparin during HD (3). We described a case of SSR in a 29-year-old hemodialysis patient. CASE A 29–year-old hemodialysis patient was admitted to our Emergencey Department. He described a left upper abdominal and left shoulder pain, nausea, vomiting and dizziness. The pain described a constant and dull pain. The patient developed severe left upper abdominal pain two days prior to admission. No association of this pain with meals, or change in bowel habits was observed. There was no history of recent trauma. He had a history of hypertension and urolithiasis since 6 years. The patient was having HD two times a week. On examination, the fever was present (37.8 oC) with a blood pressure of 80/40 mmHg and pulse rate of 120/minute. The abdominal examination was significant for pain with deep palpation in the left upper quadrant. There was voluntary guarding in this area and flank tenderness on palpation. The bowel sounds were normal. Rectal examination was normal and the stool was negative for blood. Laboratory evaluation showed a white blood cell count of 22000/ µl. Haematocrit, haemoglobin and platelet counts were 19.1%, 6.4 g/dl and 320x109/l respectively. Prothrombin time and activated partial thromboplastin time were 74% 14.7 sec (normal: 70-120%, INR 1.26) and 42 sec (normal: 26.5-40 sec) respectively. The levels of serum urea, creatinin and potassium were 202 mg/dl, 19.3 mg/dl and 8.5 mmol/l respectively. An electrocardiogram showed normal sinus rhythm. Abdominal X-ray demonstrated a non-specific bowel gas pattern. An abdominal ultrasonography showed a hyperechogenic mass (132x78.6 mm) which was composed of spleen and perisplenic fluid (Figure 1), another mass (55x66x45 mm) containing internal echogenities and moderate amount of free fluid was present in the pelvic abdomen. Abdominal parasynthesis was done and free blood in the peritoneal cavity was observed. After rapid fluid and blood infusions, the patient was taken for urgent laparotomy that revealed gross hemoperitoneum (about 1500 cc) and generalized bleeding from the surface of the ruptured spleen and splenectomy was performed. Gross examination showed a dark-gray spleen with capsular tear and subcapsular haematoma on the medial side. Microscopy revealed dilatation of sinuses, increased fibrinous tissue and hemosiderin pigments. He received intravenous cefotaxime, benzylpenicillin and further fluid resuscitation. Pneumovax vaccine was applied and intermittent haemodialysis continued. The postoperative course was uneventful and the patient was discharged from hospital on the 5th day. DISCUSSION The diagnosis of atraumatic splenic rupture was very challenging in this patient. The classic signs of abdominal pain, left shoulder pain, and shock were confounded by the other medical problems of malignancy, ascites, multiple abdominal operations, and chemotherapy (9). The SSR has been unusually shown in HD (2-4) and peritoneal dialysis (5,6) patients. Many causes and concurrent illnesses have been related to SSR in the medical literature. It was reported that pathologic rupture of the spleen had occurred almost exclusively in adults and the ruptured spleens were generally moderately to severely enlarged in a review including reported cases since 1861. The primary risk factors for SSR were splenic infiltration by a hematologic disease, splenic infarcts, and coagulation disorders, male sex, adulthood, and severe splenomegaly (10). In the previous studies, SSR related to rubella (11) and angiosarcoma of the spleen (12) were also reported. Dialysis patients with CRF show a fibrinolysis defect at the level of plasminogen activation. Reduced fibrinolysis may be responsible, along with other factors, for the development of thrombosis, atherosclerosis and their thrombotic complications (13). Kobayashi et al (14) determined that hypercoagulability and secondary hyperfibrinolysis occurred in CAPD patients. However, abnormal haemostasis is also common in CRF and is characterized by a tendency to abnormal bleeding and bruising. Prolongation of bleeding time, decreased activity of platelet factor III, abnormal platelet aggregation and adhesiveness, and impaired prothrombin consumption contribute to the clotting defects. Elevated levels of plasma guanidinosuccinic acid, by interfering with activation of platelet factor III by adenosine diphosphate (ADP), contribute to the impaired platelet function in CRF. Creatinine may cause adverse effects following conversion to metabolites such as sarcosine and methylguanidine (15). In the general population, patients with splenic infarct under age of 40 years typically have associated haemotologic disorder. In elderly patients, thromboembolic disease predominates, but is uncommonly encountered (16,17). Gascon et al (2) reported a case of a diabetic elderly man on haemodialysis who developed splenic rupture secondary to splenic infarct. Splenic infarction usually occurs in association with emboli of cardiac origin or haemotologic disorders, but in three diabetic patients on peritoneal dialysis it was due to atheromatous disease of splenic artery (8,18). The SSR is a rare complication of anticoagulants (19) or thrombolytic therapy (20). Thus, a coagulopathy produced by the anticoagulants appeared to be the only possible predisposing factor for splenic rupture (21). Hypertension is the most common complication of end-stage renal disease. Since fluid overload is the major cause of hypertension in uremia, the normotensive state can usually be restored by aggressive ultrafiltration with dialysis. Nevertheless, because of hyperreninemia, some patients remain hypertensive despite rigorous salt and water restriction and ultrafiltration (15). We detected a hypertension in our patient. The underlying cause for the SSR may be uremic coagulopathy and hypertension. Splenic rupture should be considered in any patient with abdominal pain and shock, regardless of a history of trauma or previously known risk factors for spontaneous rupture. Free fluid on abdominal ultrasound in a hypotensive patient should be considered to be blood until proven otherwise, even in a patient with known ascites (9). While the diagnosis of splenic rupture may be relatively straightforward in the trauma patient, concurrent disease in an atraumatic patient makes it a challenging diagnostic dilemma. To complicate matters, splenic rupture has been described with findings mimicking widely different problems such as cardiovascular disease and scrotal hematomas (22). Clinical symptomatology of splenic infarct and rupture consists primarily of left upper abdominal pain. Physical findings associated with splenic infarct include fever and left pleural effusion. Techniques for diagnosing splenic rupture include ultrasonography, computed tomographic scan, nuclear imaging, and angiography. The signs on CT scan include foci of hypodensity or hyperdensity that are not enhanced with contrast, and intracapsular, perirenal, and intraperitoneal fluid (23). Pre-existing ascites can make the diagnosis of intraperitoneal hemorrhage difficult. Although more sensitive, a CT scan requires that the patient be moved, which may be undesirable if she or he is hemodynamically unstable. Ultrasound is less sensitive in acute infarction. Once liquefaction of the infarcted tissue occurs, ultrasound becomes much more sensitive and is useful to follow the possibility of complications developing. There are potential complications of splenic infarct such as the development of pseudocyst, abscess, haemorrhage, subcapsular haematoma or splenic rupture (2,16). The ultrasound signs of splenic rupture are enlargement, displacement, double contour, irregularity of the spleen, and intraperitoneal fluid (23). An immediate abdominal ultrasound of our patient showed a moderate amount of peritoneal fluid and a hyperechogenic mass that were composed of spleen and perisplenic fluid. Three patients with uremia treated with hemodialysis, SSR have been presented previously in the literature. Zbrog et al (3) reported that SSR had occurred in young patient with uremia treated with hemodialysis and this patient had died due to severe shock. They explained that the uremic coagulopathy and the use of heparin during hemodialysis were being able to the factors predisposing to the rupture of the spleen. Lloveras et al (4) reported SSR in patient who was treated with hemodialysis. At the same time, Gascon et al (2) reported a case of a diabetic elderly man on hemodialysis who had been developed SSR secondary to splenic infarct. At operation, an extensive splenic infarct with rupture splenic and subcapsular haemorrhage had been detected and splenectomy had been performed. Because of the presence of shock and massive hemoperitoneum, a splenectomy was urgently performed in our patient. In conclusion, splenic rupture should be considered in any hemodialysis patient with abdominal pain and shock, regardless of a history of trauma or previously known risk factors for spontaneous rupture. Increased awareness of this condition would enhance early diagnosis and effective treatment. Early detection and aggressive multidisciplinary approach to the management of these patients may lead to a remarkable decrease in the mortality rates. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04034f1.jpg] |
| |||||||||

{kind=link}