 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 3, 2004, pp. 58-59 CASE REPORT COINCIDENCE OF ECHINOCOCCUS ALVEOLARIS AND GRANULOSUS INFECTIONS IN THE SAME LIVER Ömer Etlik1, Özkan Ünal1, İsmail Uygan2, Ali Bay3, Osman Temizöz1, M.Emin Sakarya1 Yuzuncu Yıl University, Faculty of Medicine, Departments of Radiology1 ,
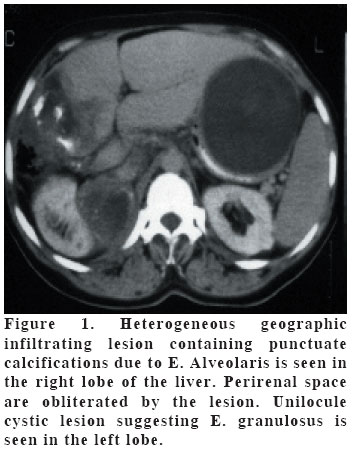
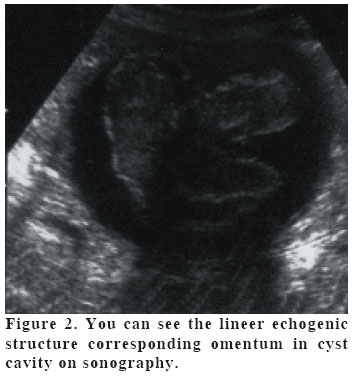
Gastroenterology2 and Pediatry3 Code Number: gm04036 We present an unusual case of involvement of the liver by both Echinococcus granulosus and alveolaris infection with typical radiological appearence. E. granulosus was located in the left lobe and the E. alveolaris was in the right lobe. To our knowledge, there is no report having both hydatid diseases of the liver so far in the literature. Key words: Liver, Echinococcus alveolaris, Echinococcus granulosus INTRODUCTION Echinococcosis is an infectious disease caused by the larval form of the genus Echinococcus. Two of the parasite species may cause severe disease in humans: E. granulosus and E. alveolaris (multilocularis). The liver is the most frequently involved organ in patients with echinococcosis. Radiological diagnosis is achieved by different methods, such as computerized tomography (CT), ultrasound examination (US) and magnetic resonance imaging (1). We reported a case with hepatic involvement by both E. granulosus and alveolaris. CASE A 14-year-old girl admitted to hospital with clinical signs and symptoms of weakness, weight loss, fever and abdominal distention. She had no a dog or cat but has ships. Her heart beat rate and temperature were normal, and blood pressure was 130/90 mm Hg. Pertinent findings included tenderness on palpation of the upper abdomen, and no cervical, supraclavicular, axillary or inguinal adenopathy. The biochemical examination of the liver function tests, ALP, direct and indirect bilirubin levels were significantly increased. US revealed uniloculer simple cystic lesion 11x10 cm in diameter with sharp margins in the left liver lobe and heterogeneous mass with calcification in the right lobe. CT demonstrated the mass involving most of the right lobe with irregular margins, which contained punctuate calcifications, and hypodense lesion with regular margin in the left lobe of liver. After the contrast material administration, the mass in the right showed no contrast enhancement, and slight capsular enhancement was seen in the hypodense lesion which was located in the left lobe (Figure 1). The lesion in the right was extended to the perirenal space and the kidney was compressed. E. alveolaris and granulosus were thought to be with typical CT and US findings before the operation. Infiltration of vena cava inferior was seen during the operation, and she was evaluated as an inoperable case. Intra-operative biopsy was performed from the lesion which was located at the right lobe. The germinative membrane of the hydatid cyst was removed and omentoplasty was made (Figure 2). E. alveolaris and granulosus were confirmed with pathological examination. Since the gastric impression, the cyst cavity was drained percutaneously with US-guidance 6 months later after the operation. The patient is still under the mebendasole treatment for both echinococosis. DISCUSSION Liver echinococcosis, the most frequently occurring form of parasitosis, is caused by the following two types of tapeworm: E granulosus and E alveolaris. We present a case with manifestation of both E. alveolaris and granulosus in the same liver. Both types are to be found in Asia, the latter even being further endemic (2,3). Imaging techniques such as CT and US enable the diagnosis to be made easily, quickly and accurately. However, US should be the primary method of investigation and is of great importance in follow-up, while CT is necessary preoperatively to assess the extrahepatic involvement. The liver is the most frequently involved organ in echinococcosis, caused by E. alveolaris or granulosus (4). Radiological findings of hydatid disease in liver are well defined (5,6). CT and US images of these two types of infections are quite different. CT appearance of E. alveolaris infections shows heterogeneous geographic infiltrating lesions without sharp margins with cystic and solid areas and may be indiscernible from malignant tumors. There is no enhancement after the contrast material administration. Amorphous or nodular calcifications are frequently present and characteristic. Venous vessel involvement, as seen in our patient, is infrequent (3). E. alveolaris has an aggressive course, and is less prevalent than E. granulosus. The diagnosis of E. granulosus infection is easier. Pathognomonic signs of the hydatid nature of a cystic lesion are visualization of the cystic wall, calcification of the cyst wall, daughter cysts, and membrane detachment (4). Although the radiologic diagnosis posses no problem when it is alone, the diagnosis may be difficult when together. In our case, because of different hepatic lobe involvement, it was not difficult. Although many hydatid diseases are reported in the literature, and both types are prevalent in Turkey (3), there is no report having both infections caused by E. granulosus and alveolaris in the same liver even though they were located in different lobes. If the patient had a cat or a dog infected by the both parasites, the togetherness would be explained easily. We think that both parasites were located in the same liver incidentally. It should be considered that both infections may be seen in the same patient and it may cause misdiagnosis. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04036f1.jpg] [gm04036f2.jpg] |
| |||||||||

{kind=link}
{kind=link}