 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 4, 2004, pp. 1-6 REVIEW ARTICLE VENOMOUS SNAKE BITE IN TURKEY FIRST AID AND TREATMENTKadir Ertem Inönü University, Turgut Özal Medical Center, Department of
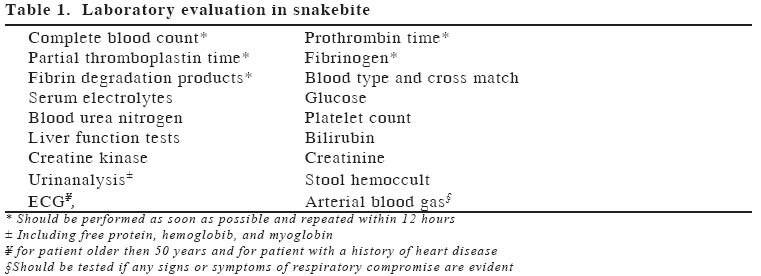
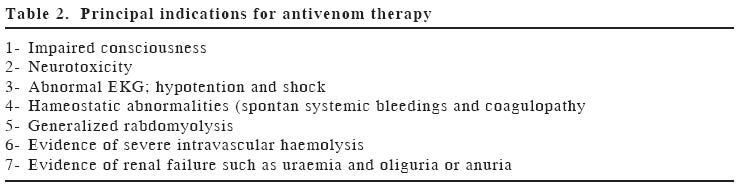
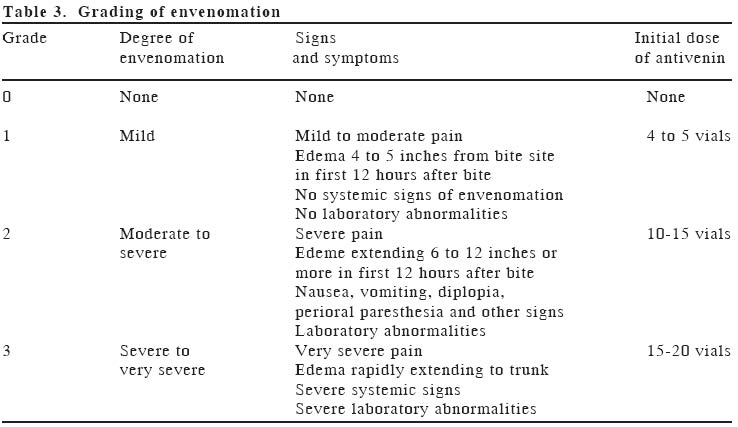
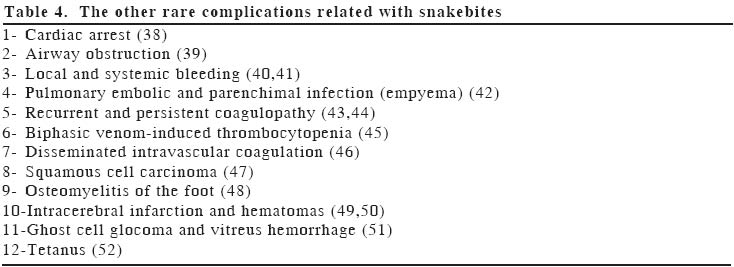
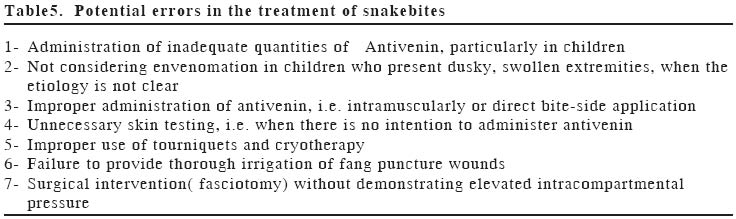
Orthopaedics and Traumatology Code Number: gm04037 In this review, we evaluated venomous snakes in Turkey, as well as the symptoms related these venomations and principles of current first aid and treatments and possible complications. Geographically, mostly vipers as most venomous snakes were found to be in Turkey. The people who work or travel in agricultural areas should be aware of venomous snakebites in this country. Generally the symptoms of victims depend on neurotoxicity, myotoxicity and coagulopathy effects in vipera envenomation. Especially, in addition to emergency room physicians, general surgeons and hand surgeons must be familiar with the principles of diagnosis and current treatment modalities for to avoid unavoidable complications as well death or limb amputations. Key words: Snake bite, venomous snakes, antivenom; toxicity, Turkey INTRODUCTIONSnakes are reptiles, and are closely related to lizards, tortoises, turtles and crocodiles. Generally, they are harmless and play important environmental roles in the fragile ecosystems of the nation's wildlife areas. They usually use camouflage and the methods like bite, hissing and buffing (1-4). Most accidental bites usually occur whenever a snake is encountered and does not have time or space to slip away. Generally, the victims were found to be bitten in the fields for example when harvesting grapes in our region. So everyone must be aware of potential dangers posed by venomous snakes when camp, hike, picnic, work or live in snake-inhabited areas. Snake bites still cause significant morbidity and mortality in developing countries. Geographically the climate of southeast region of Turkey is arid and contains mostly vipers as most venomous snakes (3-6). Venomation of vipera (Viperidea) was mostly encountered in rural areas of Turkey. Local symptoms of victims were swelling (generally appear within two hours), pain and tenderness of regional lymph nodes, bruises and necrosis on the bite side and sometimes compartment syndromes develop (digits, anterior tibial or tight). Systemic effects of envenomation: Generally epistaxis, haematemesis, echimoses, haemoptysis; subconjunctival, retroperitoneal and intracranial haemorhage may occur in case of serious clothing defects. In addition some neurotoxicity (ptosis, weakness, paresthesia, dysphagia, sweating, respiratory depression, paralysis) and myotoxicity symtoms may develop in patients with envenomed (3,5-7). Snakebite first aidIn warm climates, snakes were found to be more active. Despite many of them are non-venomous, a few of them are venomous and mostly are found to be habitatation in some cities in Turkey. Generally, when they suddenly confronted by human beings and if there is not enough time or space to slip away, they bite for to defend themselves. Anyone who is helping an envenomed victim should be aware of the envenomous snakes of the region and have a profound knowledge about the first aid approaches. Only 10 of the more than 40 indigenous in Turkey were found venomous (2). First of all the helper should determine whether the victim is envenomed or not. The symptoms and signs to look for depend on the type and amount of venom injected, bitted location, and the victim's age, body size and general health conditions. Usually, sense of extreme fright is the common reaction to a snake bite. The use of local ice packs, incision and suction and alcohol or sedative drugs for sedation of victim and pain killers such as aspirin and non-steroid anti-inflammatory drugs should be strictly discouraged. Typically, these patients may become emotionally unstable with thoughts of imminent death, or conversely, the victim may become in extreme withdrawal or lethargy state. Because of fear, victim can present some symptoms as nausea, vomiting, diarrhea, dizziness, fainting, cold, clammy skin and tachycardia. In this regard, it is important that autonomic reactions must not be mistaken for systemic symptoms and signs resulting from the snakebite. Therefore, local and systemic signs must be evaluated profoundly (4,8-10) In addition, an envenomed one should be reassured and a firm immobilization must be strictly applied to the bitted limb and keep it below the heart level. Then remove any jewelers or constricting clothes before edema occurs. A passive transportation to a safe zone can aid to calm the victim and can also diminish the spread of venom by circulation. With applying a 5-15cm creep bandage proximal to the wound can impede lymphatic flow. Generally compressive bands are not advocated for retarding the arterial and venous circulation (4,7,10-13). However, Bates recommended the tight (arterial) tourniquets for rapidly acting neurotoxic venoms (for example, bites by the mamba, krait, coral snake, Egyptian and Cape cobras) (4,7). Ralidis recommended that the use of various incisions can only be allowed when prompt medical treatment is more than 30 minutes away (10). Sutherland et al showed that pressure alone or immobilization alone did not delay venom movement in their study with monkeys. It could be possible to diminish the venom movement only with application pressure and immobilization to victims'snakebite limb (14). Generally electric shock therapy (often with a stun gun) is of no use and could cause serious injury and was discouraged by many authors (8, 12,15,16). Venom pump extractor can be beneficial if applied in few minutes (3-5min) after the snakebite (8,10,12,17). Bush et al studied about the negative effects of venom extraction device and no benefit was demonstrated, but showed skin necrosis associated with the device (18). Despite usually the snakes in Turkey are not so venomous to kill a victim, but some complication related snake bite were found to be local necrosis on bite side, neurotoxicity, myotoxicity and serious clothing defects can complicate the case's clinic (2,3). At the hospital, the victim must have supportive care related with ABC management, pain medication (avoid sedatives for it can obscure neurototoxicity symptoms), tetanus prophylaxis should be considered under immunized or non-immunized cases, wound care, and broad-spectrum antibiotics. A detailed recommendation for laboratory evaluation for a snakebite victim should be accomplished routinely summarized in Table 1 (12). Gold et al. presented a useful list of indications for antivenom treatment (Table 2) (19). If local and systemic signs of envenomation obviously have been found, the victims must have antivenin that selected according to VDK (Venomous Detection Kite) as an antidote immediately (20). Envenomation grading and antivenin administrationAntivenin is derived from antibodies created in a horse's serum when this animal injected with the snake venom. Anyone who is using this drug in an envenonated victim can encounter some rare but unavoidable allergic conditions such as fatal anaphylactic shock (1). The patient's bitten area in the limb must be followed closely and should be graded according to severity of symptoms related with extremity edema, and laboratory abnormalities during the first day following the snakebite (Table 3) (9). Antivenin constitutes the major role especially in envenomed grade II-IV victims (9,21). In addition moderate and severe grade victims; antivenin can be used for mild bites with progression of local symptoms (22). The use of polyvalent antivenom is found to be safe and effective associated with prompt improvement in the patient's condition. Acute allergic reactions were found to be generally mild and usually of urticaria in clinical trials (23,24). In the last decade we encountered some developments in antivenin drugs. The new antivenin called CroFab (Savage Laboratories, Melville, NY) was found to be less frequently occur low acute reaction (urticaria, broncospasm, hypotension) and delayed reactions (serum sickness) according to the polyvalent antivenin (25). Despite, skin testing was generally recommended by many authors, because of the possibility of a simple allergy such as urticaria or an fatal anaphylactic reaction to the horse serum used in skin testing, this test should be applied in the intensive care units (12). Some authors recommend skin test for envenomed victims and atopic patient who has severe envenomed can have antivenin treatment with prophilactic adrenaline, as well as antihistamines and hydrocortisone administration (4,21,26,27). Shaw et al demonstrated that they could treated by aggressive use of polyvalent equine antivenin safely prevented the need for surgery in sixteen of nineteen envenomed children and recommended that moderate to severe rattle snake envenomations be treated primarily with antivenin in an intensive care unit with an initially slow rate infusion and that compartment pressures be measured selectively. They concluded that surgery for rattlesnake bite is indicated for the patients who have confirmed compartment syndrome that refractory to antivenin treatment (28). Some authors was also supported the treatment of snakebite envenomations mainly by antivenins with superior survival and preservation of muscle function (29,30). In this regard, Gold et al demonstrated an envenomed patient who has a compartment syndrome (detected intracompartmental pressure was 55mm Hg) that could be treated by large doses of neutralizing antivenom given concomitantly with mannitol and hyperbaric oxygen (31). Better et al showed the amelioration of intracompartmental pressure with using IV hypertonic mannitol in an experimental study in dogs (32). Prophylactic antibiotic administration Most physicians recommend a broad spectrum antibiotic use in especially in moderate and severe grade envenometed victim (8,9). Blaylock was recommended antibiotic ointment on localized lesions (13). However, LoVecchio et al were treated fifty-six patients with rattlesnake envenomed. Only % 6 patient had antibiotics treatment and they did not detect any infection from the snakebite wounds and concluded that prophylactic antibiotics are not indicated in patients with rattlesnake bites (33). As well as Kerrigan et al found that there is no use of prophylactic antibiotic for prevention of infectious complications of crotalid envenomation (34). Breiner especially emphasized on wound hygiene only unless documented cellulitis found. He does not ratify ice packs, heating packs too and were found to be more harmful than beneficial (35). Surgical treatmentNowadays, in sake of better first aid and emergency department treatment facilities, new better antivenoms with low side effects and wound healing factors are all decreased the number of surgical interventions. However surgery occasionally is still indicated. Breiner emphasized that too urgent debridement may cause more harm than good. Generally, we see a blister and erythema on the bite location as a soft tissue respond to snakebite that may appears immediate or delayed up to 2 or 3 days. Radiation from this small blister is a zone of erythema of 2 to 3 cm with the bite mark becoming the center of the "bull's eye". Generally, instead of cellulitis, this erythema represents a local immune response. The erythematous process may spread up to 3 to 5 cm and over the ensuing days, the blister will turn into a necrotic eschar (generally 5 to 7 days after the envenomation injury) (35). Fasciotomies are generally recommended in case of the clinical symptoms related with compartment syndromes (marked swelling, hyperesthesia, tenseness, and pain on passive finger stretching of the lesion located side upper or lower limb). However, routine intracompartmental pressure at the snake-bitted limb should be measured with catheters in most clinical practice. If this measurement is greater than 30mm-45Hg, fasciotomy can be accomplished for surgical decompression (7,9,21,36). ComplicationsSerum sickness, because of the deposition of immune complexes, is a recognized complication of the administration of foreign solutions such as antivenins. The possibility of this complication and its related symptoms and signs should be explained to the patients clearly who had antivenin treatment before to discharge, so it can be recognized and treated more early. The most frequently encountered late complication is serum sickness (type III hypersensitivity) that occur approximately 5-24 days after the administration of antivenom and generally manifested by fever, urticaria, itching, periarticular swelling, albuminuria, rashes, arthralgias, and lymphadenopathy as well as rarely a peripheral neuritis, pericarditis, or encephalitis (4,8,37). The Other rare complications related with snakebites are summarized in Table 4. Errors in Treatment There are some mistreatment approaches that may influence the victim's morbidity badly. Forhs et al. emphasized some errors about the treatment of snakebite that summarized in table 5 (9). ConclusionIn addition to emergency room physicians, general surgeons and hand surgeons must be familiar with the principles of diagnosis and current treatment modalities for to avoid unavoidable complications as well death or limb amputations. REFERENCES
The following images related to this document are available:Photo images[gm04037t4.jpg] [gm04037t5.jpg] [gm04037t3.jpg] [gm04037t2.jpg] [gm04037t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}