 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
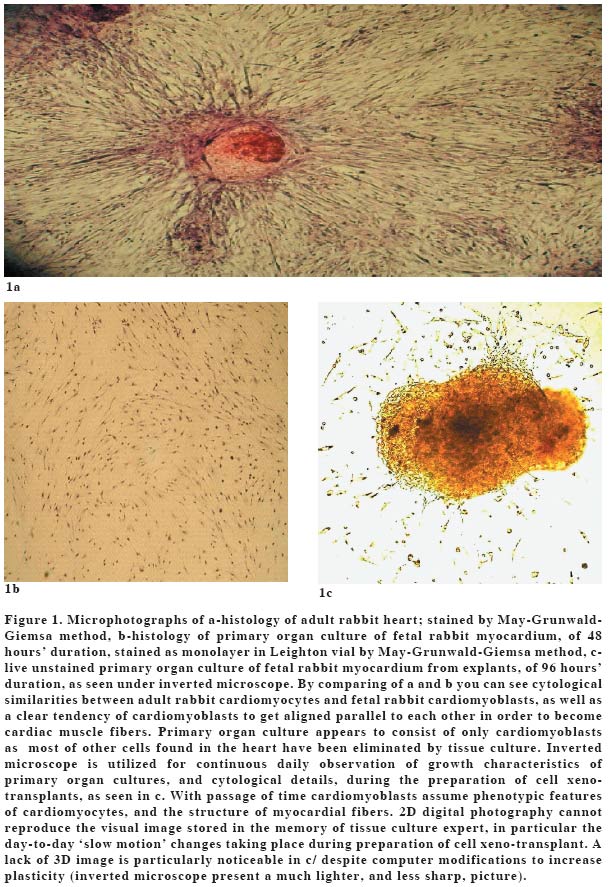
REVIEW ARTICLE STEM CELLS AND MYOCARDIAL REGENERATIONE. Michael Molnar Bio-Cellular Research Organization, Barksdale Professional Center Code Number: gm04038 Cardiomyocytes lose their ability to proliferate after birth and so heart muscle fibers cannot regenerate. For that reason myocardial injury, such as myocardial infarction (MI), heals by replacement of contractile heart muscle fibers by fibrotic tissue scar, which not only cannot participate in pumping of blood, it does not even contribute to passive mechanics of heart. Massive loss of cardiomyocytes after MI is a common cause of heart failure (HF), which is a consequence of many other cardiovascular diseases, and serious public health problem. Now……Abundant experimental data about the ability of implanted myoblastic cells to restore function of damaged cardiomyocytes encouraged interventional cardiologists in Paris, France, and Dusseldorf, Germany, to treat patients with extensive myocardial infarction by cell transplantation (CT). Due to paucity of suitable donors for orthotopic heart transplantation, and severity and risk of such undertaking, success of cell transplantation in prevention of massive damage of heart muscle after MI has been encouraging. Cell transplants used in the above clinical trials were autologous: skeletal myoblasts in Paris (1), mononuclear bone marrow cells in Duesseldorf (2). The Duesseldorf group reported clinical data of 10 patients after MI treated with their method of cell transplantation + standard therapy, compared with parameters of 10 patients receiving standard therapy only. After 3 months' follow-up the post-MI scar, measured by left ventriculography, was decreased significantly within CT group, and was significantly smaller than in standard therapy group. Infarction wall movement velocity increased significantly in CT group only. Dobutamine stress echocardiography, radionuclide ventriculography, catheterization of the right heart, all showed a significant improvement in stroke volume index, left ventricular end-systolic volume, contractility, and myocardial perfusion of the infarct region (3).Due to limited availability of human fetal cardiomyocytes alternative sources of suitable cell transplants for treatment of myocardial infarction, congestive heart failure, dilate cardiomyopathy, and other heart diseases, have been searched. A single fiber of skeletal muscle retains skeletal myoblasts beneath basal lamina throughout lifetime. From these myoblasts skeletal muscle regenerates in case of injury. In two rat models of heart failure allogeneic skeletal myoblasts were injected into four myocardial sites. Within 3 days donor single skeletal fibers disappeared, while their myoblasts began to differentiate into multinucleated myotubes. This process took 4 weeks, and caused a significant improvement of cardiac function (4). A group of rats that received intramyocardial injection of ex vivo for 7 days expanded autologous skeletal myoblasts, 7 days after infarct, had significantly better left ventricular function than controls during 2 months'follow-up, and somewhat better than the group treated by ACE inhibitors alone, as assessed by 2D echocardiography. The best results were in the group that received simultaneously CT and ACE inhibitors (5). In a rat model of myocardial infarction an intra-infarct injection of allogeneic skeletal myoblasts 7 days after MI improved post-MI in vivo exercise capacity, and ex vivo global ventricular dilation and septum-to-free wall diameter, determined by pressure volume curves obtained from isolated, red cell perfused, balloon-in-left ventricle hearts, 3 and 6 weeks after cell transplantation. As much as 13 out of 14 hearts showed evidence of survival of transplanted myoblasts (6). In a pig model of myocardial infarction, 2 weeks after MI an intra-infarct injection of autologous mesenchymal stem cells from bone marrow was done. Two weeks after transplantation, a robust engraftment in all treated animals, with expression of muscle-specific proteins, attenuation of contractile dysfunction, and marked reduction of the extent of wall thinning measured by piezoelectric crystals placed in the myocardium before MI was observed (7). As an alternative to skeletal myoblasts, allogeneic fetal cultured stomach smooth muscle cells were transplanted in a rat model of MI. All animals were immunosuppresed by cyclosporin A. Transplants formed smooth muscle tissue in the infarcted myocardium and improved contractile function as compared with controls. Angiogenesis was apparent as well (8). Embryonic cells injected into infarcted myocardium of a rat model of MI presented their new cardiomyocyte phenotype by strong positive staining to sarcomeric alpha-actin, cardiac alpha-myosin heavy chain, and troponin I, 6 weeks after cell transplantation, at which time a significantly improved cardiac function was measured, too (9). Clonal stem cell line WB-F344 from a male adult rat liver was injected as cell xenogeneic transplant into the left ventricle of adult female nude mice. Male WB-F344 cells with the same genotype were identified within the implantation site 6 weeks later. Phenotype of these new ' stem cell derived cells'was that of cardiomyocytes. So adult liver-derived stem cells responded in vivo to the tissue environment of adult heart and differentiated into mature cardiomyocytes (10). Autologous skeletal myoblasts have been favored in clinical practice to-date because of easy availability. In reality due to lack of connexin43, gap junction protein, skeletal myoblast transplants should not be as effective as cardiomyocytes to treat MI. Only connexin43 containing cardiomyocyte transplants build intercellular connections with host myocardial fibers, such as gap junctions and desmosomes, and thereby act synchronously with the host heart. Neonatal cardiomyocytes of 3 days'old rats were injected into the border zone of infarct 10 days after injury. Subsequently, from 4 to 14 days later on, treated hearts were studied by immunohistochemistry. Antibodies against connexin43, desmoplakin, and cadherin, identifying gap junctions, desmosomes, and adherens junctions, respectively, were found between grafted cardiomyocytes, as well as between grafted and host cardiomyocytes. Grafted cardiomyocytes were seen aligning parallel to, and establishing electrical pathways with, the host cardiomyocytes (11). In two adult X-linked muscular dystrophy dogs, lacking an expression of dystrophin in both cardiac and skeletal muscles, fetal canine atrial cardiomyocytes, including also sinus nodal cells, were injected into the left ventricle. Four weeks later a catheter ablation of AV-node was carried out. Immediately thereafter a ventricular escape rhythm emerged, which originated from a new pacemaker within the labeled cell transplantation site. This was the first in vivo evidence of electrical and mechanical coupling between allogeneic donor cardiomyocytes and host myocardium (12). A comparison of fetal cardiomyocyte and skeletal myoblast transplantation in a rat model of MI showed no difference in left ventricular ejection fraction, but it was significantly lower in control group of untreated animals. All animals were immunosuppressed (13). In a comparative study of effects of transplantation of fetal ventricular cardiomyocytes, enteric smooth muscle cells, and skin fibroblasts, in a rat model of MI, 4 weeks after injury, above cell transplants were injected into myocardial scar. End-diastolic volume, +dP/dt, and -dP/dt, were all significantly higher in group of rats receiving fetal cardiomyocytes. All animals were immunosuppressed (14). Results of autologous skeletal myoblast and dermal fibroblast transplantation were compared in a rabbit chronically injured heart model: both contractile skeletal myoblasts and non-contractile fibroblasts improved structural properties of injured heart, as reflected in diastolic performance, but only skeletal myoblasts enhanced systolic performance of terminally injured heart (15). How soon after MI should cell transplantation be done? Following two studies are not in full agreement but indicate that CT should be carried out no later than 6 days after MI. When carried out by selective coronary catheterization and infusion of myoblasts, rather than injection into infarcted myocardium, CT can take place at the time of initial balloon angioplasty, stenting or other invasive procedure. In a rat model of MI fetal cardiomyocytes were transplanted immediately, 2 weeks and 4 weeks, after myocardial injury. At 8 weeks, studies of heart function, planimetry, and histology were carried out. Inflammatory reaction was greatest during the first week and subsided during the second week after MI. Scar size increased up to 8 weeks after MI. Cardiomyocytes transplanted immediately after MI were absent at 8 weeks and the scar size and heart function were as in untreated group. Cardiomyocyte transplantation should be carried out immediately after the inflammatory reaction is over, but before the scar expansion (16). Ultrastructural analysis of infarcted myocardium in murine model of MI showed a complete loss of damaged cardiomyocytes within 2 days and healing by scar within 7 days after MI. Implanted cardiomyocytes were engrafted throughout the wall of infarct already two weeks after MI, with their excitability intact, and their differentiation proceeding at fast pace (17). The fate of cardiomyocytes injected into infarcted myocardium of adult rat model of MI, 7 days after injury, was followed by a quantitative TagMan PCR, and histology, and heart function was evaluated by biplane angiography. Grafted neonatal cardiomyocytes were still present 6 months after transplantation, they thickened left ventricular wall, and significantly increased ejection fraction and reduced paradoxical systolic bulging of the infarcted area (18). Previous studies with bone marrow stromal cells engrafted into xenogeneic fetal recipients were repeated: the recipients were fully immunocompetent adults, and no immunosuppression was used. Bone marrow stromal cells were taken from C57B1/6 mice and injected into adult Lewis rats. One week later the recipients underwent coronary artery ligation and were sacrificed 1 to 12 weeks thereafter. Labeled mice cells were engrafted into bone marrow cavities for the duration of experiment. Circulating mice cells were found only in rats with 1-day old MI. Mice cells were found in the damaged myocardium by immunohistochemistry. This study proved that adult stem cells engraft into a xenogeneic live being, without immunosuppression, without difficulty. Simultaneously, they can home to injured myocardium, differentiate into cardiomyocytes, and create a stable chimera in the heart (19). Human mesenchymal xenogeneic stem cells were injected into the left ventricle of CB17 SCID beige adult mice without immunosuppression. After 7 days, de novo expression of desmin, beta-myosin heavy chains, alpha actinin, cardiac troponin T, and phospholamban, all typical of cardiomyocytes, could be detected. Human adult xenogeneic mesenchymal stem cells engrafted in the myocardium and differentiated into cardiomyocytes (20). Embryonic cardiac cells were cultured for 3 days, and then implanted 7 days after extensive MI into myocardium in a rat model, without immunosuppression. Engrafment of cell xenotransplants was observed 1, 4 and 7 weeks after CT. Differentiation of embryonic cells into cardiomyocytes was proven by antibodies against alpha -SMA, connexin43, and fast and slow myosin heavy chain. Serial echocardiography revealed that CT prevented scar thinning, left ventricular dilatation and dysfunction as compared with controls (21). Some reports about experimental use of stem cell transplantation list angiogenesis as one of the benefits. Using rat model of MI, allogeneic aortic endothelial cells were injected into myocardial scar 2 weeks after infarct. Transplanted cells stimulated angiogenesis, increased perfusion in the myocardial scar, but there was no improvement in overall heart function (22). …and then….For years transplantation of placental cells has played for major role in therapy of arteriosclerotic vascular disease, because placenta cells cause generalized vasodilatation, overall circulatory improvement, and increased budding of capillary collaterals. While developing corneal transplantation, Prof.Dr. Filatov searched for a method to avoid post-operative clouding of corneal transplants. Once during such operation he implanted tissue fragments of placenta subcutaneously. Corneal clouding did not occur, and implantation of placental cells became a major topic of Soviet research institutes, and soon spread to the West as "Filatov treatment". Experimental study on treatment of arteriosclerotic vascular disease by placenta cell transplantation reports also on clinical application of the same treatment (23). Scientific explanation why placenta cells have been the most widely used cell transplants to-date is limited. Embryonic stem cell research will undoubtedly provide answers because of the close relationship between embryonic stem cells and trophoblastic cells. Without trophoblasts embryo could never become a newborn. At the beginning of conception trophoblasts are indistinguishable from ' embryonic stem cells'. Only at the stage of 58-cell human blastocyst can the outer cells, destined to produce trophoblasts of placenta, be recognized as different from the inner cells, which will form embryo. In 107-cell human blastocyst, 8 embryo-producing cells are surrounded by 99 trophoblastic cells, a 12: 1 numerical discrepancy (24). The advances in therapy of myocardial infarction and heart failure, as well as other heart diseases, based on the initial experimental work of groups of Chiu RC (1995), Li RK (1996), and Menasche P (1996), were preceded by a several decades long clinical experience of German practitioners of cell therapy, and Soviet cell transplantologists. Since 1953 there were yearly national symposia in Germany, where theoreticians and practitioners of cell therapy exchanged ideas and discussed results. In 1954 Therapiewoche in Karlsruhe attracted 5,000 physicians practicing cell therapy. There is up to 2,000 publications about cell therapy since 1953 in various German medical journals. The summary of those most important was published in 1975 by International Research Association for Cell therapy in Frankfurt: "Literaturverzeichnes der Internationalen Forshungsgesellschaft fur Zelltherapie". In USSR there were biannual all-USSR cell transplantation symposia since 1976 until 1990, and a lot of publications, but reports prior to 1970's are hard to find. The sole publication in English (25), a translation of the same book in German of 4 years earlier (26), presents the scientific basis of cell therapy. In the above book there is a report about treatment of 251 cardiac patients with cell therapy, of which only one got worse, the rest were improved or unchanged: in 35 patients 3 -6 months post-MI the success rate was 51%, in 76 patients with various types of myocardial damage success rate was 53%, in 41 patients with "myodegeneratio cordis" success rate was 72%, in 9 patients with conduction block of Adams-Stokes type success rate was 55% (27). This was before the era of routine heart catheterization and interventional cardiology, and other modern technologies: none of the above patients received cell transplants via injection into damaged myocardium or via balloon catheter in the branch of coronary artery. Fetal cell xenotransplants were implanted deeply subcutaneously, counting on homing of these fetal progenitor cells into injured tissue, and their differentiation into cardiomyocytes and vascular cells. The concept of homing was proven in 50-ies in Germany by isotope and intravital dye studies (25, 26, 28, 29), and since 1993 also in other western countries. (30, 31, 32) Publications about treatment of diabetes mellitus, and its microangiopathic complications, by islet cell transplantation, are more numerous than for any other illness in which CT is indicated. It is remarkable that no one has ever thought to transplant islet cells directly into pancreas of a diabetic patient. Usually the implantation was into the liver, directly (very rarely), indirectly via portal vein (used only in urgent situations), or indirectly into liver via portal vein-vena cava anastomotic system above umbilicus (commonly used). Liver is the most immunoprotective organ in the body: no live cell implanted directly into liver is ever rejected. This well established scientific fact, has never been explained. In islet cell transplantation for diabetes mellitus the idea of homing has been accepted for decades. In 1993 the author gained first clinical experience with cell transplantation in cardiology. In a cooperative study of International Institute of Biological Medicine in Moscow and Russian Research Institute of Pediatrics of Russian Academy of Medical Sciences 7 terminal patients with dilated cardiomyopathy, aged 4 to 14 years, were treated by human fetal cell transplantation. Cell transplants of myocardium, liver, and placenta, were implanted under the aponeurosis of rectus abdominis muscle above the umbilicus. One patient of 10 years of age died four days after cell transplantation: autopsy found that dilated cardiomyopathy was secondary to anomalous origin of coronary arteries. The remaining patients benefited from the procedure, were able to return home in improved condition, which was entirely unexpected. One of patients got worse one month later at home, was admitted to the Coronary Care Unit of the local hospital, and died. Besides homing, cell therapy in Germany and cell transplantation in USSR, have
been based on the following concepts. Only fetal cells are used for transplantation -with
the exception of cell transplants of various endocrine glands where neonatal
cells have been utilized. Their Stem cells from fetus are much more numerous than rare adult stem cells, so that no special cell isolation procedures have to be utilized in preparation of cell transplants. In fetus stem cells live in milieu of various already differentiated cells. Fetal stem transplants contain other cells of the same family, of various generations, and in cell-to-cell contact. Primary benefit of cell transplantation is direct stimulation of regeneration of damaged cells of the recipient rather than replacement of destroyed cells. Only small children in early stages of their illness are treated by one cell transplant only. The usual chronically ill patient requires transplantation of cells of all those organs or tissues which are involved in the pathophysiology of patient's disease(s). The more exact is the pathophysiological and biochemical diagnosis the more accurate will be the choice of cell transplants for treatment. Cardiac patients have usually received besides transplant of myocardial cells also cells of liver and placenta (and lungs in cases of left side heart failure with pulmonary congestion and hypertension), unless additional malfunctions are discovered which could be corrected by transplants of cells with necessary compensatory functions. No immunosuppression is required in clinical application of cell transplantation. Of estimated 5 to 25 million patients treated by cell transplantation worldwide , 99.99% underwent allogeneic or xenogeneic transplantation without immunosuppression. In its approbation of islet cell transplantation for clinical practice in 1984 the Ministry of Health of USSR stated under 4/ that no immunosuppression is necessary, providing that guidelines for preparation of cell transplants are followed: namely the use of primary cell culture. Of 22 recent studies described in this paper (1 -22), in 5 dealing with cell xenotransplantation no immunosuppression was used, and in 12 about allogeneic CT the authors utilized immunosuppresssion in 3 studies only. Cell transplants can be prepared for patient treatment from any vertebrate, from Homo Sapiens to fish. The sole exception is frontal lobe of the brain which animals lack, and so frontal lobe cell transplants have to be of human fetal origin. For obvious ethical, moral, religious, and practical, reasons only cell xenotransplantation has been used in Germany and other western European countries until recently. In USSR human fetal tissue transplantation was abandoned after 1988 in favor of xenotransplantation. The scientific basis for the use of cell xenotransplantation has been the principle of "organospecificity". Key cells of the same organ or tissue are the same in Nature, regardless of the species of origin, e.g. they are organ-specific (or tissue-specific) and not species-specific, and the same applies to any of over 200 kinds of cells found in human or animal body. In 1898 E.B. Wilson described his observation that in various genera the same organs always originated from the same group of cells, e.g. organospecificity (33). There are no antigenic differences between the corresponding cells of identical organ of different animal species (and man), and cell surface antibodies are organ-specific (or tissue-specific) and non-species specific. This is another proof of organospecificity (34, 35, 36). Organospecificity has been ' res ipsa loquitur' for German and USSR cell transplantologists. Development of molecular cell biology during the last century was based on the fact that all eukaryotic cells in Nature are built and function according to the same laws. Great majority of proteins from different organisms (including man) is similar over the entire amino acid sequence, e.g. they are homologous of each other (37). Since 1987 the author used solely fetal cell xeno-transplants of rabbit origin, prepared by primary organ culture. In Figure 1 compare microphotographs of histology of rabbit adult myocardium (a), with histology of primary organ culture of rabbit fetal cardiomyoblasts after 48 hours (b), and with the same primary organ culture as seen live unstained in inverted microscope, after 96 hours (c). After reviewing Figure 1 find pictures of human adult and fetal myocardium in any standard histology and embryology textbooks and be surprised by morphological similarities between human and rabbit myocardium. ……..and in the futureAutologous cell transplantation, of skeletal myoblasts, or mononuclear bone marrow stem cells, directly into damaged myocardium, is a reliable treatment for patients with serious myocardial infarction, or heart failure, who do not need cell transplantation immediately to save their life, and are hospitalized in a top hospital, with qualified invasive cardiologists, and excellent tissue culture laboratory. If this therapeutic method should become important for the health care system worldwide, stem cell xeno-transplantation will probably have to be utilized. Stem cell xeno-transplants can be delivered to any hospital without delay, at all times, and transplanted indirectly into liver if interventional cardiologist is not at hand, without immunosuppression. Subsequently such patient can be transferred to the high level hospital for the specialist's care. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04038f1.jpg] |
| |||||||||

{kind=link}