 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
ORIGINAL ARTICLE A STEREOLOGICAL STUDY ON AZUROPHILIC AND SPECIFIC GRANULES IN NEUTROPHILS OF PATIENTS WITH SCHIZOPHRENIA BEFORE AND DURING ANTIPSYCHOTIC TREATMENT Ibrahim Mohammed Inuwa1, Nona Viernes 2, Ziad Zaidan2 Sultan Qaboos University, Departments of Human and Clinical Anatomy1and
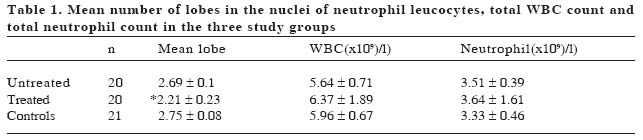
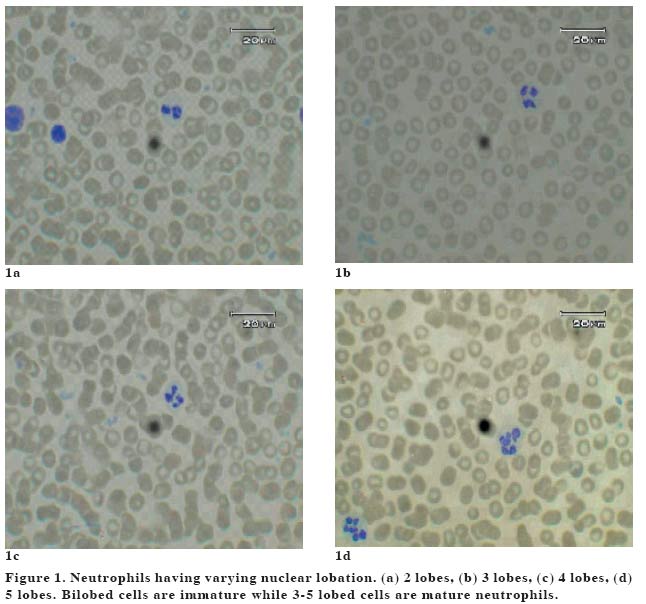
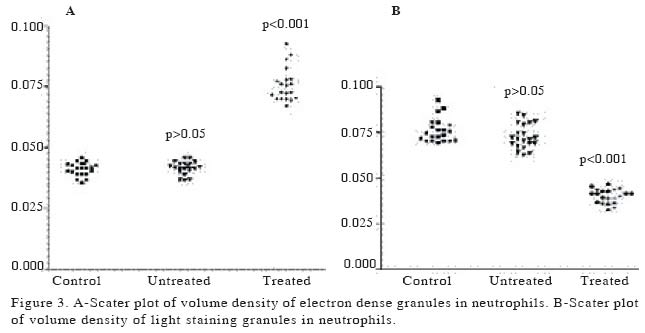
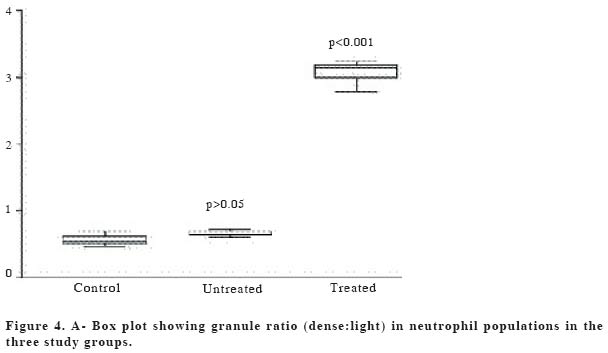
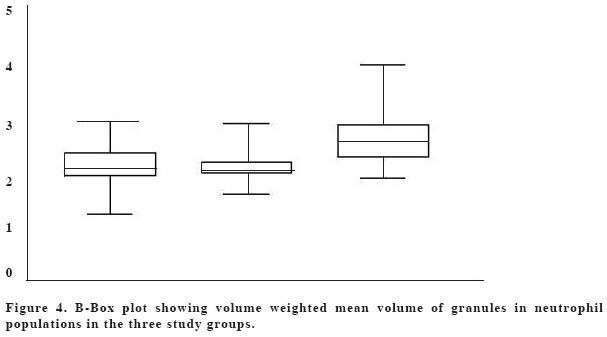
Behavioural Medicine2 Code Number: gm04039 Antipsychotic drugs, frequently used for treating schizophrenia, have many unpleasant and sometimes life threatening side effects. Some of these side effects, such as agranulocytosis cannot be explained satisfactorily on the basis of the drugs' pharmacological actions. The first indication of this event is neutropenia which then progresses to full blown agranulocytosis. This study was carried out to quantitatively assess neutrophil maturity in patients on antipsychotic drugs using the appearance of their granules on electronmicroscopy. Blood samples were collected from schizophrenic patients (n = 20) before and six weeks after starting treatment with two types of Antipsychotic drugs (Risperidone and Chlorpromazine) and from healthy subjects (n = 21) having no history of antipsychotic drugs medication and processed for transmission electron microscopy. Volume density of azurophilic (electron-dense) granules in patients after treatment was found to be greater than both before treatment and in control group. The volume weighted mean volume of granules was significantly greater in cells of patients after treatment. There were significantly more neutrophils with fewer than three lobes of nuclei in patients after treatment than in controls or before treatment. These findings suggest neutrophil cellular immaturity in the patients during 6 weeks of treatment even though there was no haematological evidence of neutropenia. It is suggested that immaturity of neutrophils manifests before any evidence of neutropenia. Key words: Schizophrenia, antipsychotics, neutrophils INTRODUCTIONSchizophrenia is a chronic debilitating psychiatric disorder. Its etiology is not well understood and probably consists of several separate illnesses. Symptoms include disturbances in thoughts, affects, and perceptions and difficulties in relationships with others. The hallmark symptom of schizophrenia is the experience of auditory hallucinations. The mainstay of treatment on this condition is by the use of antipsychotic drugs (1-3). These drugs fall into two categories; conventional ones such as chlorpromazine and unconventional ones such as clozapine. The mechanism of action of these drugs is believed to be through their anti-dopaminergic activity specifically dopamine D2 receptor antagonism (4,5). Conventional antipsychotic drugs are associated with adverse effects, such as sedation, dystonia and muscle stiffness, tremors, elevated prolactin levels, and weight gain (6). Many patients with negative symptoms of schizophrenia do not respond to conventional antipsychotic drugs which may necessitate the use of atypical antipsychotic ones (7). Although the use of atypical antipsychotic drugs is associated with marked improvement in the symptoms of schizophrenia, their use is linked to the increased risk of development of agranulocytosis, which can occur in about 1% of patients (8,9). This side effect is usually unpredictable and consequently, frequent monitoring of WBCs is required in such patients (10). During human neutrophil differentiation, large portions of the genome condense and associate with the nuclear envelope to form filament-like structures. As a result, the nucleus of the mature neutrophil typically consists of a linear array of three or four lobes joined by thin, DNA-containing filaments. Nuclear segmentation is therefore an indicator of maturity of neutrophils (11). At electronmicroscopy, the appearance of neutrophil granules are used as indicators of maturity as well. There are two types of granules in the neutrophil based on their electron density; light staining granules are predominantly found in mature cells whereas dark staining (azurophilic) granules are predominantly found in immature cells (12). Stereological morphometry has been used by many workers on normal and pathological tissue to obtain quantitative structural information that may have physiological or biochemical correlates (13-15). The majority of stereological parameters are ratios such as volume density, or absolute quantities such as total volume, surface area, length etc (16). Stereological morphometry is a powerful tool because it provides a three-dimensional information which makes interpretation of functional morphology more effective This study used light and electronmicroscopic stereological methods to evaluate maturity of neutrophils in patients on treatment with antipsychotic drugs before any laboratory evidence of the onset of neutropenia in such patients. MATERIAL AND METHODS Experimental designPatients recruited in the study were newly admitted with the diagnosis of schizophrenia. The diagnosis was made using the DSMIV criteria (Am Psych Assoc. 1994). After appropriate consent from the next of kin was obtained the patients were clinically examined for obvious evidence of infection. Blood samples taken for total blood counts (CBC). Those patients found to have evidence of active infection were excluded from the study. Within a period of six months, 20 patients satisfied the inclusion criteria and were used for the study. The control group were a similar number of age-matched subjects who were not taking any sort of medication at the time of the study. At day 0, (before the start of treatment) 2 millilitres of venous blood was obtained from each patient. Patients were then treated with clozapine (300 mg/day) or risperidone (6 mg/day) for a period of 4 to 6 weeks. At the end of 6 weeks 2 millilitres of venous blood was again obtained. Complete blood count (CBC) in patients was monitored routinely every week throughout the six weeks of treatment. Light microscopyTwo millilitres of venous blood sample obtained was placed in heparinised containers from each patient and control subject. A drop of the heparinised blood was placed on a glass slide and a thin blood film was made. The blood film was fixed with 70% acetone and stained with Giemsa stain. One hundred systematic random sample of neutrophils per patient were evaluate for nuclear lobation according to Arneth Cooks criteria (17). Transmission electronmicroscopy One millilitre of the blood sample was placed in a 2ml tube centrifuged down, the white blood cell layer (buffy coat) was removed, and suspended in buffered Karnovski fixative (Ph 7.26) for 30 minutes. The suspended cells were converted into a pellet (1mm3) by centrifugation at 1500 rpm using a bench top refrigerated micro centrifuge (Sanyo Hawk). The cell pellet was then postfixed in 1% osmium tetroxide dehydrated in increasing acetone series, and embedded in Araldite. Semithin sections obtained with a Leica ultracut microtome were stained with toluidine blue so as to identify appropriate cell types. Silver sections were then obtained, mounted on copper grids, double-stained with uranyl acetate and lead citrate (18) and observed in a Zeiss EM900 transmission electronmicroscope. StereologyAll stereological estimates were obtained using Histometrix software (Kinetic imaging Ltd) attached to an IBM personal computer. Measurements were made on digitized images of neutrophils obtained from the electronmicroscope. Granule volume density was estimated using the point counting method by randomly throwing test points oparison post ten the micrograph (19). Volume weighted mean volume of granules was estimated using the point-sampled intercept method (20). Data was reported as group mean +/- standard error of the mean. Difference between patient groups was analysed using paired student t test while difference between patient groups and controls was analysed using ANOVA with Neuman multiple comst. Mean difference was considered to be statistically significant if P was found to be less than 0.05. RESULTSMean numbers of nuclear lobes in neutrophils are shown in table 1. Amongst the control group, nuclei of 90.4 % of cells had between 3-5 lobes whilst 9.3 % have less than 3 lobes. In the untreated patients, 91.9 % of cell have nuclei that have between 3-5 lobes and 8.1 % have less than 3 lobes (Fig 1). After six weeks of treatment, 29.6 % of the neutrophil population of the patients were found to have 3-5 lobed nuclei and 70.3 % had less than 3 lobed nuclei (p<0.05). The total and differential white blood cell counts in all the three groups were within normal range for the general population and were not significantly different from one another (see Table 1). Volume density of electron dense granule (Fig 2) populations in controls was 0.0408 ± 0.001 (s.e.m), whilst that of light staining granules was 0.0714 ± 0.001 (s.e.m). Volume density of electron dense granule populations was significantly higher in treated group than in untreated group and control (p<0.001). There was no significant difference (p>0.05) in volume density of both groups of granule populations between controls and untreated groups (Fig 2). Mean ratio between electron dense and light staining granules in each cell was 0.526 ± 0.19 (s.e.m) in the control group. This ratio was significantly increased (p < 0.001) in treated group when compared with controls and untreated groups. No significant difference (p > 0.05) was found between controls and untreated group (Fig 3). Average granule volume weighted meanvolume regardless of type was 2.223± 0.09 (s.e.m) µm3 in control group, 2.167 ± 0.05 (s.e.m) µm3 in untreated group and 2.706 ± 0.11 (s.e.m) µm3 in treated group. Granule volume weighted mean volume was significantly greater (p < 0.001) in treated patients as compared to untreated (Fig 4a)(Fig 4b). DISCUSSION Our data has demonstrated that total white blood cell count and neutrophil count in untreated patients and those treated for six weeks were not significantly different from controls. However, a significant percentage of those neutrophils in treated patients have bilobed nuclei. This is an indication of immaturity and suggests that the bone marrow is releasing cells before the nuclei are completely segmented. Such bone marrow response is usually secondary to an increase in demand due either peripheral neutrophil destruction or malignant transformation (21,22). Neutrophils have two distinct granule populations; azurophilic staining granules which are large and appear as electron dense granules on elecronmicroscopy, and specific granules which are small and appear as light staining granules on elecronmicroscopy. Azurophilic (primary) granules are more abundant in immature cells than specific (secondary) granules (23). Our data on granule volume density, granule ratio, and absolute volume weighted mean volume correlated positively with the light microscopy finding of immaturity. In the absence of any source of infection, or other pathologic condition that could explain the observed neutrophil morphology, these findings could be a consequence of drug treatment. An equally important question to ask is if these effects on neutrophils are due to drug treatment, then, what is the likely mechanism involved? The mechanism of action of antipsychotic drugs used in treatment of schizophrenia is believed to be through their antidopaminergic effect. It could it be possible that their anti dopaminergic activity is the basis of the observed neutropenic effect. Sookhai et al (24) have demonstrated the presence of dopamine receptors in neutrophil populations of normal human volunteers. These receptors are the D2 family (D2,3,4) which are known to be the sites of activity of antipsychotic drugs. However, in the same report, the investigators found that stimulation of the receptors with dopamine agonists induced apoptosis in neutrophils. Therefore the immaturity of neutrophils observed in our study could not satisfactorily be explained on the basis of drug-receptor interaction -if anything, the antipsychotic drugs being antidopaminergic should not cause neutropenia! Loeffler, et al (25) have suggested that the observed neutropenia and subsequent agranulocytosis is due to enhanced apoptosis of blood neutrophils resulting from enhanced expression of the pro-apoptotic proteins Bax and Bik and from a decreased expression of the anti-apoptotic BCl-X(L) mRNA. The antipsychotic drug commonly associated with the highest risk of agranulocytosis -clozapine is known to undergo bioactivation to a chemically reactive nitrenium ion. This ion has been suggested by Williams et al. (26,27) to be the agent responsible for neutrophil apoptosis through a mechanism of cell surface haptenation and glutathione depletion. Another possible explanation for immaturity of neutrophils could be due to direct intracellular accumulation and subsequent cytotoxicity. It could be that the drugs preferentially accumulate inside neutrophils causing cell death which leads to a reactive myeloblastic response of releasing more immature cells into the circulation. A structure-activity relationship model using physicochemical parameters such as lipid solubility, ionic charge and molecular weight of drugs developed and used to determine where substances will accumulate inside cells (28) has shown that, antipsychotic drugs have the properties that will make them accumulate inside mitochondria of cultured fibroblasts. It could well be possible that these drugs accumulate intracellular preferentially in neutrophils causing mitochondrial toxicity and subsequent cell death. Indeed it has been observed that mitochondria of patients treated with antipsychotic drugs were swollen and had disrupted cristae -features indicating direct organelle injury (29). In conclusion, although it has long been acknowledged that the use of antipsychotic drugs is associated with a risk of unexplained agranulocytosis, it is suggested here that a likely mechanism of this effect is through direct selective neutrophil toxicity possibly involving mitochondrial destruction and subsequent cell death. The earlier indication of this effect could be the presence of immature neutrophils in peripheral blood without associated evidence of neutropenia. It is therefore suggested that patients treated with antipsychotic drugs particularly the atypical ones should have their neutrophil granulocytes assessed for maturity even if there is no haematological evidence of neutropenia. AcknowledgementWe are grateful to the Sultan Qaboos University for funding this project, and to the nurses of psychiatric ward of Sultan Qaboos University hospital for assistance with blood sample collection. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04039f3.jpg] [gm04039f4a.jpg] [gm04039f1.jpg] [gm04039t1.jpg] [gm04039f2.jpg] [gm04039f4b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}