 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 4, 2004, pp. 29-35 ORIGINAL ARTICLE SERUM CYSTATIN C: A GOOD MARKER FOR EVALUATION OF GLOMERULAR FILTRATION RATE IN HEPATORENAL SYNDROME Amgad E. El-Agroudy 1, Alaa A. Sabry1 , Hosam A. Ghanem2, Ayman El-Baz3, Ashraf Fakhry3, Hosam M. Gad 1, Hussein A. Sheashaa 1, Mohamed Abdel-Hamid4, Mahmoud Yousseff4, Abd El-Rahman A. Mokhtar4 Mansoura University, Urology & Nephrology Center1, Clinical Pathology
Department2, Medical Biochemistry Department3, and General
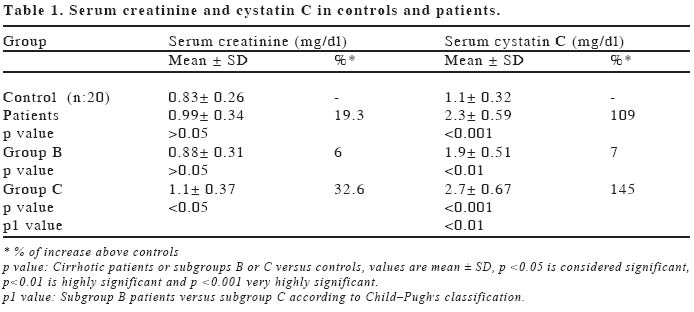
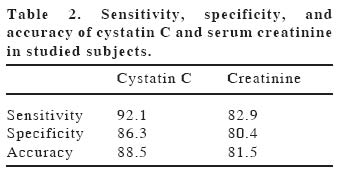
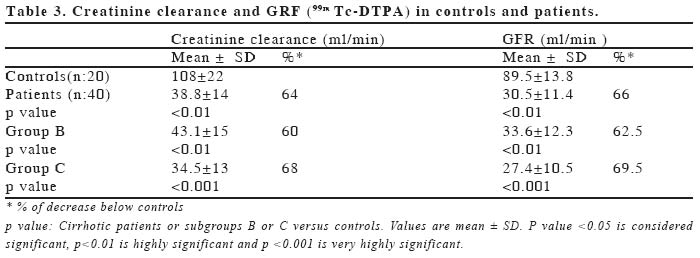
Medicine Department4 Code Number: gm04041 To determine if estimation of serum cystatin C could replace creatinine clearance in routine determinations of glomerular filtration rate (GFR) for early detection of kidney affection in patients with cirrhosis in a case control study. 40 patients with cirrhosis were included in this study according to Child-Pugh's classification, 20 patients (group C) and 20 patients (group B). Twenty adults aged, sex and body mass index matched were used as controls. Serum creatinine and creatinine clearance were measured by Jaffe reaction. GFR was measured by 99m Tc-DTPA technique. Serum cystatin C was measured by particle enhanced immunoturbidimetry. Pearson correlation analyses showed that cystatin C has no correlation with age or body mass index. Moreover, cystatin C showed more significant correlation r = -0.85, p <0.001, than serum creatinine r = -0.32, p <0.05 with GFR measured with 99mTc-DTPA technique in patients with cirrhosis. The results demonstrated that serum cystatin C values were significantly higher in hepatorenal syndrome patients than in controls. Results showed that neither serum creatinine nor creatinine clearance were good indicators of hepatorenal syndrome(r = 0.089). Serum cystatin C level is independent of age or body mass index. Thus we suggest that serum cystatin C assay may be useful marker for early detection of renal insufficiency in hepatorenal syndrome. Also, the increase in cystatin C is higher in decompansated cirrhotic patients than in compensated cirrhotic patients. Key words: Cystatin-Glomerular Filtration Rate-Hepatorenal syndrome INTRODUCTIONHepatorenal syndrome (HRS) is defined as a clinical condition that occurs in patients with advanced cirrhosis, characterized by impaired renal function and marked abnormalities in the arterial circulation and endogenous vasoactive systems of the kidney (1). There is marked vasoconstriction, which results in low glomerular filtration rate (GFR), while in the extrarenal circulation; there is predominance of vasodilatation, which results in reduction of total systemic vascular resistance and arterial hypotension (2). HRS may also develop in patients with other chronic or acute liver diseases. The diagnosis is established as described by International Ascites Club. Diagnostic criteria of hepatorenal syndrome proposed by the International Ascites Club. Only major criteria are necessary for the diagnosis of hepatorenal syndrome). Major criteria include: (i)Low GFR as indicated by serum creatinine greater then 1.5 mg/dl or 24-hour creatine clearance lower than 40 ml/min,(ii)Absence of shock, ongoing bacterial infection, fluid losses and current treatment with nephrotoxic drugs,(iii)No sustained improvement in renal function (decrease in serum creatinine to 1.5 mg/dl or less or increase in creatinine clearance to 40 ml/min or more) following diuretic withdrawal and expansion of plasma volume with 1.5 L of a plasma expander,(iv) Proteinuria lower than 500 mg/day and no ultrasonographic evidence of obstructive uropathy or parenchymal renal disease. Serum creatinine and creatinine clearance (Cr Cl) are the most widely accepted methods for non-invasive estimation of GFR in clinical practice to diagnose patients with hepatorenal syndrome (1), and elevations in serum creatinine are often the initial presentation of renal complications. However, serum creatinine concentrations are poor guide to GFR since they are highly dependent on extra-renal factors such as muscle mass, gender, age, protein intake and inflammation and interference by several compounds such as protein, bilirubin, acetoacetate etc. during estimation (3,4). Because the accurate measurement of urine volume is very difficult even in research studies (4,5), the actual measurement of creatinine clearance is decreasing in clinical practice. It is suggested that an ideal renal filtration marker should be freely filtered at the glomerulus, neither reabsorbed nor secreted along the nephron, produced at a steady state and eliminated only by the kidney. Thus much more reliable and specific markers of GFR, alternative to creatinine, are required (6) Cystatin C is a non glycosylated, low molecular mass (13 KDa) basic protein that is a member of the cystatin superfamily of cystatin protease inhibitors (7). It consists of 120 amino acids and is produced by all nucleated cells, and even in inflammatory conditions, the production rate is unaltered (8). The low molecular mass of cystatin C and its high isoelectric point allow it to be freely filtered by the glomerular membrane. Also, its stable production rate suggests that cystatin C may be a potential new marker of GFR (9). Several investigations have been suggested that cystatin C concentrations in serum correlate well with glomerular filtration rate (9-11). The aim of this study is to evaluate the suitability of cystatin C for the diagnosis impaired renal function, and if it is better diagnostic marker than creatinine to diagnose and monitor hepatorenal syndrome. For this purpose, we measured serum creatinine, 24 hours creatinine clearance, renal GFR (99mTC-DTPA clearance) in patients with cirrhosis and compared them with the results of serum cystatin C to be evaluated as a better diagnostic marker of renal function. MATERIAL AND METHODSPatients This study was performed in sera of 40 patients with cirrhosis who were hospitalized for therapy in General Medicine Department, Mansoura University Hospital. Patients with decompansated stage of cirrhosis were included in the study. According to Child-Pugh's classification (12), 20 patients were in group C and 20 patients were in group B. Our study patient group comprised 30 males and 10 females with a mean age of 47.5 years. All the patients had low serum albumin level (mean ±SD; 2.43±0.40; reference range: 3.5-5.0g/ dl), some with mild ascites and others with more advanced disease. The ascites duration of these cases varied between 6 months and 4 years. Atrophic liver, dilatation of the portal and systemic veins, splenomegaly, and ascites were detected by ultrasonography and esophageal varices were determined by the endoscopic examination. The liver cirrhosis in most of the patients developed following viral hepatitis; in 10 cases HBsAg, in 23 cases Anti HCV, and in 7 cases both HBsAg and Anti-HCV was positive. All of the cases were previously diagnosed histopathologically. In general, the clinical presentation of our patients with cirrhosis was ascites. At least 1 week before the study, diuretics and other drugs were stopped. All of the cases were evaluated for any superimposed conditions such as chronic obstructive lung disease, congestive heart failure, coronary heart disease. Patients who developed hepatoma, gastrointestinal bleeding, spontaneous bacterial peritonitis or encephalopathy were excluded from the study. All cases were administered a standard low sodium diet (40 mmol/day) during the study. Twenty healthy subjects (15 males and 5 females) with fully normal biochemical parameters were selected and served as a control group with the mean age of 46.8 years. Blood samples were obtained after an overnight fast and divided into (1) 1 ml of blood with sodium fluoride for blood glucose, (2) 5 ml of blood into plain tubes, left 20 min at 37 oC and unhemolyzed serum was separated for albumin, bilirubin, AST, ALT, creatinine and cystatin C. Complete 24 hour urine was collected for protein assay and creatinine clearance. Glucose measurement was done by glucose oxidase method (BioMerieux, France). AST, ALT and bilirubin assay was done by spectrophotometric Kits (BioMerieux, France) using autoanalyzer (Synchron LX, Beckman, USA) Total urinary protein was measured by turbidimetric method (Stanbio Laboratories, San Antonio, Texas, USA) while urinary albumin excretion was measured by enzyme immunoassay (Orgen Tec Diagnostic Gmbh, Germany). Serum Cystatin C assays:Serum cystatin C assay was made by latex particle enhanced turbidimetric immunoassay PET kit (13,14) (Dako, Glostrup, Denmark). Cystatin C PET kit contains polystyrene particles of uniform size, chemically coupled with rabbit antibody against human cystatin C. A reaction between these immunoparticles and cystatin C in a patient specimen results in the formation of agglutinates and a concomitant change in the absorbance signal. The cystatin C concentration of the patient specimen is determined by interpolation on a calibration curve. Creatinine assay and creatinine clearance:Serum and urinary creatinine concentration were determined by Jaffe reaction (15). Creatinine clearance was calculated from the urine and serum creatinine (16) for this purpose, 24-h urine specimens were collected from all of the patients and controls. GFR determination:GRF measurements had been made on these patients according to the single injection technique using 99mTC-DTPA (99mtechnetium diethylenetriamine pentaacetic acid). After overnight fast the patients were ingested 5 ml/kg water and basal blood samples were obtained. 99mTc-DTPA was given I.V. in a dose of 4 m ci for adults. Three clearance collection periods of 20 minutes duration were done. Blood and urine samples were obtained at the beginning and end of each collection period and 99m Tc-DTPA activity was measured (17). Statistical analysisStatistical analyses were performed on an IBM compatible personal computer using the statistical package for social scientists (SPSS) for windows 9.0 (SPSS Inc., Chicago Il, USA). Pearson correlation coefficient was used for determination of correlation between renal parameters studied p value of < 0.05 was considered statistically significant. Sensitivity, specificity and accuracy of cystatin C and creatinine were calculated. The following calculations were made: sensitivity (true positive÷[true positive+false negative]), and specificity (true negative÷[true negative+false positive]). The accuracy was calculated as true positive+true negative divided by the total number of patients (15). RESULTSOn investigation of the parameters of renal functions in the studied group, mean values of serum sodium levels were 129.7± 5.9 mEq/L. Mean values of serum cystatin C is significantly higher in patient group than in controls. The increment above control for serum cystatin C in total studied patient group and in subgroup B and C according to child Pugh's classification was much higher than serum creatinine. Mean value of serum cystatin in group C is significantly higher than in group B (Table 1). Serum cystatin C showed higher sensitivity and specificity than serum creatinine in the studied subjects. The highest sensitivity of cystatin C was at cut off value 1.2 mg/L for patient group while the highest sensitivity of creatinine was at cut off value 0.8 mg/dl in the control group (Table 2).Mean values of GFR (99mTC-DTPA) in the patient group was significantly decreased compared to the controls (p<0.001) (Table 4). The mean creatinine clearance value (38.8 ml/min) was found to be significantly higher than GFR (30.5 ml/min) measured by Tc-DTPA (p<0.05) (Table 3). Serum cystatin C showed higher significant negative correlation with 99mTc-DTPA than serum creatinine (Table 4). On the other hand, serum cystatin C showed no correlation with the body mass index (r: 0.20, p>0.05) or age (r:0.13, p>0.05). So, the best correlation of GFR (Tc-DTPA) was found with serum cystatin C (r:0.86) in control group, No significant correlation was found between creatinine clearance and GFR (r:0.089, p>0.05). DISCUSSIONIn clinical practice, serum creatinine is the most widely used method for non-invasive estimation of GFR to diagnose patients with hepatorenal syndrome (1). Using serum creatinine and creatinine clearance seems not to be satisfactory to assess renal function in hepatorenal syndrome. Thus it is clear that new and more specific tests are required. It should also be noted that creatinine production is closely related to muscle mass. Muscle mass and GFR are dependent on age, both tending to fall with increasing age. Because of the several difficulties on collection and preserving the urine, calculation of creatinine clearance causes well know problems in older patients. In addition measurement of body weight accurately may be difficult, due to difficulties on quantitating ascites and edema in these cases (6). The more sensitive, accurate and reproducible the measure of function, the more expedient and directed can be the management response. The constancy of glomerular filtration rate (GFR) under physiological conditions and the fast that it is affected by the majority of disease processes involving the kidney have led to its wide acceptance as one of the best indices for the measurement of renal function (18). The ideal marker for GFR determinations would appear endogenously in the plasma at constant rate, be freely filtered at the glomerulus, be neither reabsorbed nor secreted by renal tubule, and undergo no extra renal elimination. These characteristics can be useful benchmarks for comparing the advantages and disadvantages of new methods for GFR measurement (19).When we evaluated the tests for renal function the best correlation of GFR (Tc-DTPA) which is gold standard for this study was found with serum cystatin C. This agrees with Demirtas et al. (20). It has been known that there are some difficulties in applying the GFR (Tc-DTPA) test in advanced cirrhotic patients. By contrast, cystatin C may be measured automatically on various analyzers in sera in several minutes with a great precision (8). Also, GFR measurement by radionuclide method provides an accurate method but their use is limited by the inherent restriction associated with the clinical use of radioisotopes. In the present study, mean values of serum cystatin C were 1.1±0.32 mg/ L for controls. Helin et al. (21) reported that children over one year age had 1.33±0.63 mg/L level and similar to that for adults. Also, in the present study, serum cystatin C levels showed no significant correlation with age (r: 0.13, p >0.05 or body mass index r:0.20, p>0.05).Filler et al. (22) demonstrated age independence of cystatin C in children below 18 years and an upper reference value of 1.38 mg/L and these results are similar to those of adults value reported by kyhse-Andersen et al. (23). However, the small differences between these studies can be explained by the different calibrator material used in the different studies (11). Cystatin C is produced by all nucleated cells and its production rate is unaltered in inflammatory condition. So, cystatin C is not an acute phase reactant (24). Cystatin C is almost completely reabsorbed, catabolized and broken down in the cells of proximal convoluted tubule. It is practically entirely filtered via the glomerular membranes without any significant tubular secretion. Its stable production rate combined with low MW strongly indicates that serum concentration mainly determined by GFR (9). The results of this study demonstrated that neither serum creatinine nor creatinine clearance were good indicators of hepatorenal syndrome, as they have no significant correlation with GFR (Tc-DTPA) results. Decreased serum creatinine in their study explained by several ways such as under production of creatinine in diminished muscle mass or decreased rate of hepatic production of creatine, which is the precursor of creatinine because of the destruction of hepatic cells in these patients (20). As well as cystatin C being unaffected by the interfering conditions mentioned above, it has also been shown that cystatin C is not an acute phase reactant (24) and is less expensive than the GFR (Tc-DTPA) test. Thus, it seems to be a reliable, fast and easy to use marker of renal failure. In the present study, cystatin C showed high sensitivity than creatinine in detection reduced GFR in hepatorenal patients. These results are similar to those reported previously (25). On the other hand, Filler et al (12) reported no difference between cystatin C and creatinine for estimating GFR. This controversy in results could be due to difference in selection of patients and various nephropathies covered. Moreover, Herget-Rosentnal et al.(10) reported that higher sensitivity and negative predictive value of cystatin C are equivalent in patients with glomerular or tubular impairment. In the present study, cystatin C showed higher increment above control than serum creatinine in early stages of kidney affection of hepatorenal syndrome. A mild degree of renal dysfunction may develop unnoticed as creatinine level may remain in the normal range despite a major decline in GFR, and the use of serum creatinine may inaccurately estimate GFR due to dietary intake, tubular secretion of creatinine (11,12). In the present study, cystatin C showed more significant correlation than serum creatinine with GFR by 99mTc-DTPA techniques. These results confirm those noticed by Coll et al (25). They reported that serum cystatin C levels started to increase when GFR was 88 ml/min/1.73 2m, while serum creatinine level began to increase when GFR was 75ml/min 1.73 2m. These data indicate that serum cystatin C may detect mild reduction in GFR than serum creatinine. Wang et al.(26) reported close correlation between creatinine clearance and 99m Tc-DTPA. On the other hand, Shemesh et al.(27) reported that creatinine clearance is of little value in estimating GFR. In a prospective study on 23 non-azotemic cirrhotic patients whose mean GFR (inulin) was 32 ml/min, similar results were found reporting that the serum creatinine level failed to rise above normal even when the GFR (Tc-DTPA) was very low (less than 25 ml/min). The same study demonstrated that creatinine clearance overestimated inulin clearance by a factor of 2 (28). On the other hand, increased creatinine clearance with decreased GFR has been reported in patients with several types of renal failure (18). Demirtas et al. (29) found that cystatin C is a more sensitive marker then creatinine in evaluation renal toxicity induced by cisplatin therapy in oncologic patients. Newman and price (30) have suggested cystatin C as the best endogenous GFR marker. In conclusion, serum cystatin C concentration is independent of age or body mass index. Cystatin C may be a useful marker for early detection of renal insufficiency in hepatorenal syndrome for which early treatment is important. Thus, cystatin C might be a superior marker of GFR evaluation compared to creatinine and might be added to routine renal tests for hepatorenal syndrome. Also, the increase in cystatin C is higher in decompansated cirrhotic patients than in compensated cirrhotic patients. REFERENCES
The following images related to this document are available:Photo images[gm04041t3.jpg] [gm04041t2.jpg] [gm04041t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}