 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 4, 2004, pp. 36-41 ORIGINAL ARTICLE DO GENDER DIFFERENCES HAVE INFLUENCE ON PSYCHOSOCIAL STRESS, QUALITY OF LIFE AND WORK DEMANDS? CROSSSECTIONAL STUDY Giedrius Vanagas1,2, Susanna Bihari-Axelsson2 1Kaunas University
of Medicine, dept. Preventive Medicine, Kaunas, Lithuania 2Nordic
School of Public Health, Gothenburg, Sweden
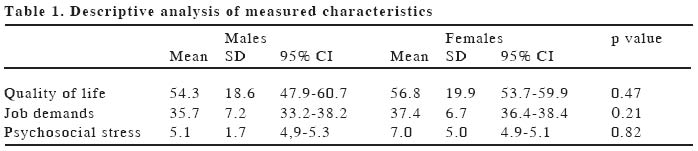
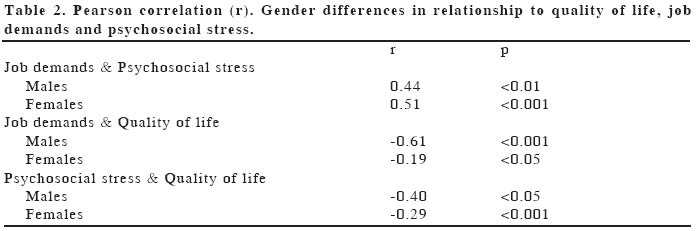
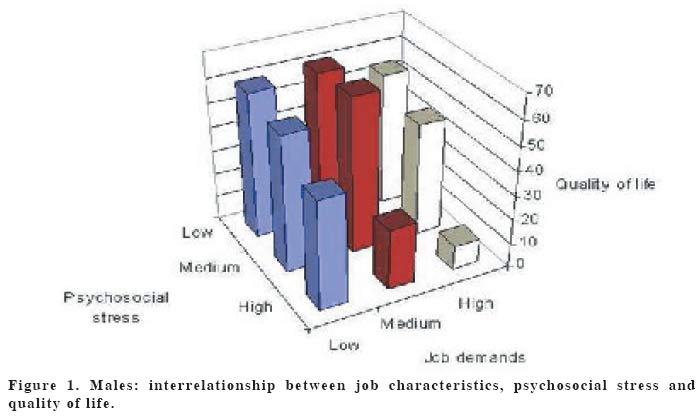
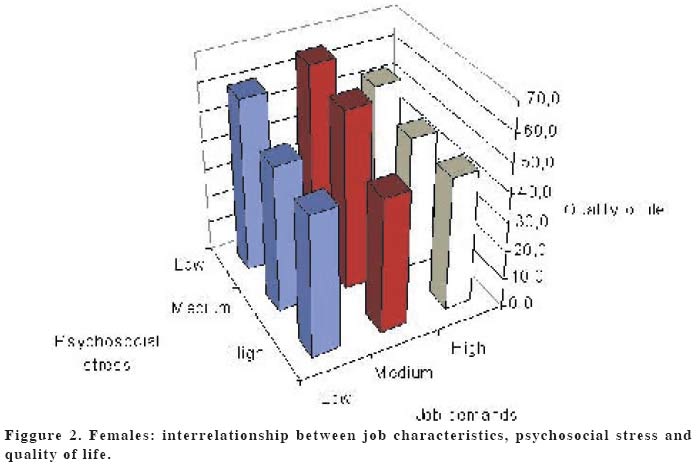
All over the world studies have argued that general practice has become an increasingly stressful work because of increasing demands and constraints. As a consequence of the health reform in Lithuania there have been changes regarding the role and tasks of GP's. These changes have led to new job demands that may affect the quality of life for the Lithuanian general practitioners. There may also be gender differences in this respect. Cross-sectional study of 300 Lithuanian general practitioners. A visual marked scale to asses quality of life. Psychosocial stress was investigated with a questionnaire based on the Reeder scale. Job demands were investigated with the Karasek scale. There were no significant gender differences among Lithuanian GP's in quality of life (p:0.47), job demands (p:0.21) and psychosocial stress (p:0.21). Strong relationships were however discovered between quality of life and psychosocial stress (r:-0.40 and r:-0.29); psychosocial stress and job demands (r:0.44 and r:0.51);, job demands and quality of life (r:-0.61 and r:-0.19) for males and females respectively. There seems to be no significant gender difference in quality of life, job demands and psychosocial stress among Lithuanian GP's, but there are strong associations between psychosocial stress, job demands and quality of life for both genders. High job demands and high psychosocial stress for GP's predict a lower quality of life for both genders compared to those with low job demands and low psychosocial stress. Keywords: general practitioner; gender; quality of life; job demands; psychosocial stress INTRODUCTIONAll over the world studies have indicated that general practice has become an increasingly stressful work (1-8). The previous attractions of the work, such as the independence and flexibility involved in providing a service as a small business, are now being undermined by increasing demands and constraints in the work situation (3,9). According to one study, only 50% of general practitioners are satisfied with their work (3). The Lithuanian health care reform started in 1992. A primary health care development strategy has been mapped out for 1996-2005. As a consequence of the health reform there have been changes going on regarding the role and tasks of GP's in Lithuania. In 1996-1997 operational service standards for general practitioners were defined. Primary health care services are delivered in primary health care centers, GP's, both school and community medical posts (paramedical centers), ambulatories and polyclinics, women's consultancies, nursing hospitals, as well as by the ambulance service (stations and divisions). This means an increased workload and increased responsibilities for Lithuanian GP's. There are presently 1007 GP's in Lithuania and 80% of the GP workforce is female. The new demands on the Lithanian GP's may increase their work-related stress. Such stress may have serious social and psychological consequences for the GP's (10). Studies have shown that work-related stress influences the physicians'health and job satisfaction, which may have serious consequences for the patients'care and the patients'satisfaction with the quality of care. The most frequently mentioned sources of job stress for GP's were increasing workloads, paperwork, insufficient time to do justice to the job and new models and conditions of work (6). The results also point to important gender differences. Compared with their male colleagues, the female GP's experienced a higher job strain. Female GP's reported a high workload, low job control and low social support at work (11,12). Studies of Swedish GP's have shown that 12.8% of them had scores indicative of severe psychiatric disturbance and 53% had considered abandoning general practice because of occupational stress (5). There were significant associations between psychosocial working conditions and impaired quality of life in Swedish GP's (13). It is still unknown, however, how the health care reform in Lithuania influences the GP's quality of life and if it has any relationship to work demands and level of stress. The aim of this study is therefore to investigate quality of life and its relationship to work demands and psychosocial stress among Lithuanian general practitioners. MATERIAL AND METHODSTarget group: Lithuanian general practitioners. Study designCross--sectional study. A postal survey of random national samples. Computerized randomization was performed from the registry of Lithuanian physicians. The data collected through the questionnaires filled in by the GP's. Sample size; Sample size was calculated using EpiInfo 2000 Statcalc software whish argued the sample size of 192 GP's with the 95% confidence level. From the previous studies the expected response rate was 63%. Therefore, it was decided to send questionnaires to 300 Lithuanian GP's. Our observed response rate was 66%. We collected 197 filled-in questionnaires. Assessment of Psychosocial StressPsychosocial stress in this study was investigated by a questionnaire based on the Reeder scale (14). The (15,16) Reeder scale uses four statements experienced in everyday stressful situations as "usually tense or nervous", "daily activities are extremely trying and stressful". The respondents should indicate whether each of the statements describe them. Each question has four alternative responses, which were coded using Likert-like scale. A simple inversion (high stress was indicated by high rather than low scores) of the Coulson scoring system was used, giving a score of between 0 and 8 (Annex 1) (17) Respondents scoring zero were omitted from the present analysis. We have previously found analyses based on the Coulson approach to give very similar results to analyses based on the simple summation of scores (18). Assessment of job demandsJob demands were investigated with the Karasek scale (19). This model, also known as the "job strain"model. Job demands were defined by questions such as "working very fast,""working very hard,""doing so much things", and others. A four point Likert -like scale was used with the coding from 4 to 1 for series, so that the responses were summarized to give a score (20) Assessment of Quality of lifeWe used the simplest form of questioning; the respondents were simply asked to assign a numerical value between 1 and 100 on a visually marked (100 mm long) scale that reflects the present quality of life. They assigned the quality relative to the states of best imaginable and of worst imaginable state, respectively. Statistical analysisData were computed -coded and analyzed using Statistical Package for the Social Sciences for Windows version 11.0 (SPSS Inc). The analysis included descriptive statistics, Pearson correlation coefficients and interrelation analysis. Nonparametric tests were used to test for significant differences at the p:0.05 level. The Pearson correlation coefficient was used as measure of the strength of the linear relationship between two variables. It is referred to as Pearson's correlation or simply as the correlation coefficient. If the relationship between the variables is not linear, then the correlation coefficient does not adequately represent the strength of the relationship between the variables. Pearson's r range from -1 to 1. An r of -1 indicates a perfect negative linear relationship between variables, an r of 0 indicates no linear relationship between variables, and an r of 1 indicates a perfect positive relationship between variables. RESULTSDescriptive statistics Of the 197 respondents, 162 (82.2%) GP's were female, and 35 (17.8%) male. This reflects the situation in Lithuania with 80% female physicians. The GP ages ranged from 31 to 66 years (mean 44.2 years, 95% CI 42.9-45.4). Significant gender difference was found for mean age (males 47.1 years, 95% CI 43.5 -50.7; females 43.5 years, 95% CI 42.2-44.9; p < 0.03). All other descriptive measures are shown in Table 1. There were not any significant gender differences in quality of life, job demands and psychosocial stress, but significant relationships were discovered among the Lithuanian GP's between psychosocial stress, job demands and quality of life. Pearson correlationGender differences in relationship to work demands, psychosocial stress and quality of life were analyzed with the Pearson correlation coefficient. Significant strong relationships were detected for both genders and are shown in Table 2. Figures 1 and 2 show the interrelationships between job demands and psychosocial stress and quality of life. The demands and stress distribution was divided between those below the mean (low) and those above the mean high). Figures 1 and 2 show that low rate of quality of life appears to be related to job demands rather than psychosocial stress. However, for both genders, the lowest rate of quality of life was seen when there was a high level of job demands combined with a high-level of psychosocial stress. DISCUSSIONMendelson (21) summarized the vast literature on work related stress and found that the adverse effects of stress at work vary depending on the type of occupation and individual individual characteristics such as gender. It is more difficult to establish the cause of work related stress than in case of occupational injuries, which can be attributed to specific time and place. Figures vary in the studies, depending on the criteria used for diagnosis and the research instruments used. There is consistency, however, in the finding that the incidence of anxiety and depression in GPs is higher than the incidence in the general population, and it has been increasing over the past decade (22). Some studies have discovered significant gender differences in work characteristics and psychosocial stress for GP's (12,23-25). Higher job strain rates were highlighted for males (25) as well as for females (12). Our study has shown that for Lithuanian GP's there are no significant gender differences in the quality of life, job demands and psychosocial stress but significant and strong associations between psychosocial stress, job demands and quality of life were discovered. Similar results for GP's were also described in a UK and Australia (5,9) but in these studies job demands and psychosocial stress have stronger association to quality of life for males than females. Job demands for females have also stronger association in perceiving psychosocial stress. Moreover, studies have argued that job demands account for a higher amount of explained variance in adverse health outcomes (i.e. emotional exhaustion, psychosomatic health complaints) than in the two other (positive) outcome variables (i.e. job satisfaction, job involvement) (9,26-30). Generally, job characteristics like job demands appear to be important predictors for occupational burnout in health care because psychological job demands have a significant (and direct) relationship with emotional exhaustion (26). This study found that high job demands and high psychosocial stress for GP's predict a lower quality of life for both genders compared to those with low job demands and low psychosocial stress. Low rate of quality of life appears to be related to job demands rather than psychosocial stress. The same results for job demands have also been highlighted in other studies (9,13). Another interpretation of the data takes the pattern of findings at face value and suggests that the sources of variation in stress levels and quality of life can be explained, at least in part, by the characteristics of the work setting. The statistical analysis of previous studies suggests that Karasek's job strain model has value in explaining stress in general practice (9). The reporting of stress in the context of work does not necessarily mean that work is the major source of this stress. Thus, there remains the possibility that situational variables or even other job strain variables, which were not included in the Karasek's job strain model, may have an equal or even greater influence on GP's health (26). Job demands as they have been conceptualized and operationalized in several surveys would not take into account some of the major sources of stress to general practitioners such as dealing with difficult patients (8,9) Many of these problems can be related to the health care reform in Lithuania. As a consequence of this reform, GP's are required to have more competence in diagnosis and ongoing management of medical conditions. This means increased responsibilities, which may contribute to higher psychosocial stress for Lithuanian GP's. In conclusion, our study has shown that there are no significant gender differences in quality of life, job demands and psychosocial stress among Lithuanian general practitioners, but significant and strong associations were discovered between psychosocial stress, job demands and quality of life. Our results have indicated increased job demands and higher psychosocial stress for GP's, which can be interpreted as a consequence of the health care reform in Lithuania. High job demands and high psychosocial stress for Lithuanian GP's predict a lower quality of life for both genders compared to those with low job demands and low psychosocial stress. However, a low rate of the quality of life mostly appears to be related to job demands rather than psychosocial stress. REFERENCES
Coulson Scoring System 0-No response on one or more statements. The following images related to this document are available:Photo images[gm04042f1.jpg] [gm04042t1.jpg] [gm04042f2.jpg] [gm04042t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}