 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 4, 2004, pp. 48-52 ORIGINAL ARTICLE THREE-DIMENSIONAL VOLUME RENDERING IMAGING IN DETECTION OF BONE FRACTURES Ömer Etlik1, Osman Temizöz1, Ali Doğan2, Mustafa Kayan1, Halil Arslan1, Özkan Unal1 Yüzüncü Yıl University, Faculty of Medicine,
Departments of Radiodiagnostic and Orthopedi
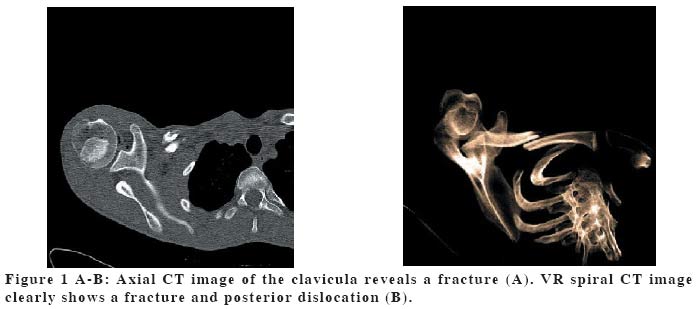
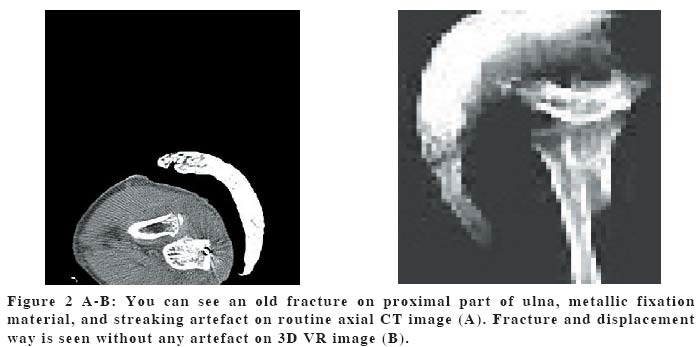
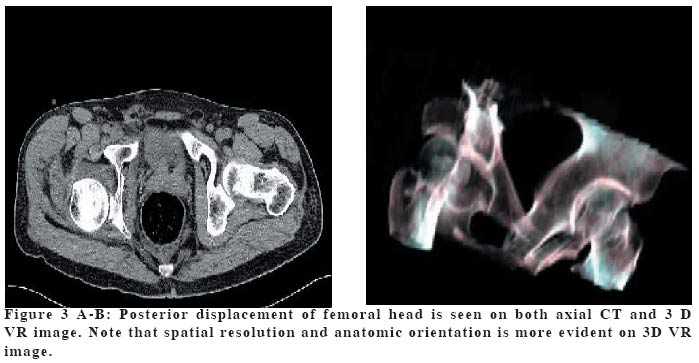
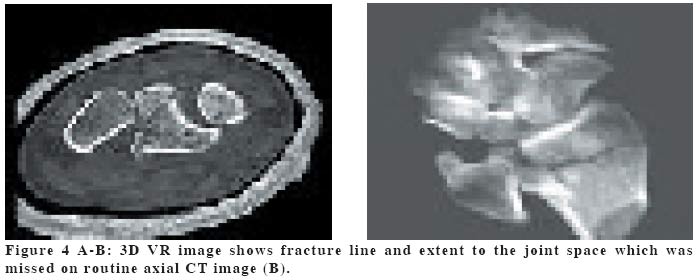
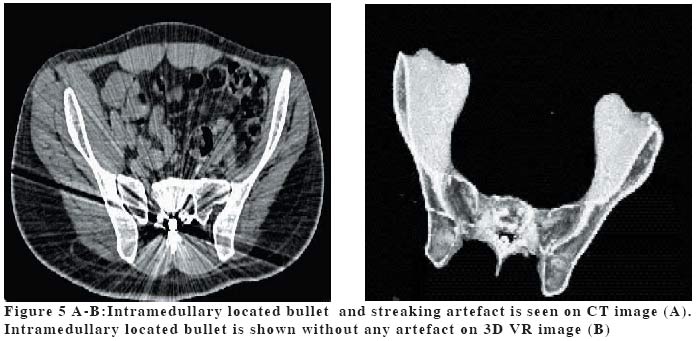
Code Number: gm04044 We aimed to evaluate the contribution of 3D volume rendering (VR) imaging findings on bone fractures. Routine CT examinations and 3D VR imaging were performed on 31 patients with bone fractures. MIP and VR images having optimal resolution in all patients were obtained using 3D reconstructions on work-station. Bone fractures and extension, bone fragment, and soft tissue changes were evaluated. Distribution of bone fractures were as follows; clavicula (n=4), radius (n=8), acetabulum (n=3), shoulder (n=4), tibia (n=6), carpal bone (n=2), sacrum (n=1) and femur (n=3). Complex fractures were seen one in scapula and 2 in pelvic region. Complex injuries, bone fragments, extension of fractures were better demonstrated with volume-rendered images. We conclude that 3D VR imaging is valuable method in detecting bone fractures and superior to other radiologic modalities. Key words: Bones injuries, Computed tomography, helical, three-dimensional, volume rendering INTRODUCTIONThe imaging of bone fractures is the most frequent work-up in radiology departments. Some imaging techniques including X-ray, computerised tomography (CT) can be used in detection of fractures. Conventional X-ray is the first step of investigation of bone fractures. But it has some limitations in detection of subtle and non-displaced fractures, and complex anatomic areas such as acetabulum and shoulder. The combination of spiral CT and 3D reconstruction with volume rendering (VR) allows rapid and detailed examination of the musculoskeletal system. 3D volume rendering images has proved valuable in diagnosis of subtle abnormalities and in planning patient therapy. In a substantial number of cases, management is altered because of findings seen only on the 3D images or better demonstrated on these images: subtle fractures, complex injuries, and pathologic conditions masked by metallic streak artefact (1-3). In this study, we aimed to detect the contrubition of 3D VR images on diagnosis of bone fractures. MATERIAL AND METHODS Initially 31 patients with bone fractures were selected for the study between April-August 2003. Nineteen of the 31 patients were man and the rest of them were woman (mean age 32±4). Multy dedector spiral CT (Siemens, Sensation 4, Erlanger, Germany) was utilised in examinations. The scanning technique was varied according to the clinical question to be answered. Small areas of interest, such as the sternoclavicular joint or the wrist, benefit from spiral acquisition of a volume data set that combines narrow collimation (1-2 mm) and a pitch of 1-1.5 with small reconstruction increments (1 mm). Larger areas of interest, such as the pelvis or lower extremity, may be examined with wider collimation (3 mm), a pitch of 1-2, and reconstruction every 2-3 mm. Creation of a 3D CT image began with the acquisition and reconstruction of axial image data. And then, axial images were sent to the work-station (Siemens, Leonardo, Erlanger, Germany). MIP and VR images were obtained using reconstructions procedure on axial image. We obtained 3D images in optimal resolution and spatial resolution like conventional X-ray in all of the patients. Two radiologists independently assessed the axial and reformatted 3D VR images. 3D images were examined in the different points of view to getting more detailed information about area of interest. We investigated the extension of fractures, bone fragman, relations to joint and soft tissue changes, and to compare the axial and 3D VR images in detection of these conditions. RESULTSA total of 87 fractures involving the clavicula (n=4) (Figure 1 A-B), radius (n=8) (Figure 2 A-B), acetabulum (n=3) (Figure 3 A-B), tibia (n=6), carpal bones (n=2) (Figure 4 A-B), sacrum (n=1) (Figure 5 A-B), and femur (n=3). The number of fractures with displacement and non-displacement was 26 and 5, respectively. Complex fractures were seen in three patients who had scapular in one and pelvic fractures in two. In these patients, the fractures and displacement and bone fragments were clearly visualised with 3D VR images. We did not observe the metallic artefact (n=6) at the evaluating of post-operative fracture. In addition, we could not obtaine the optimal images secondary to metallic artefact which was related to intraspinal metallic bullet at the S2 level in patients with gun-shoot injuries on axial CT images. But we could clearly evaluate the localization of bullet and relationship to surrounding bone without any artefact on 3D VR images (Figure 5 A-B). DISCUSSIONSpiral CT has two major roles in musculoskeletal trauma: These are to define or exclude a fracture that was equivocal at plain radiography and to determine the extention of fracture and thus provide guidance for therapy. Spiral CT will provide additional information about soft-tissue abnormalities the extension of fracture, bone fragman and soft tissue changes. But, spatial orientation can not be made optimally by means of CT images. This is the major dysadvantages of CT techniques. 3D VR techniques can eliminate the dysadvantages of both techniques, low contrast resolution and spatial resolution, X-ray and CT, respectively. On the other hand, the combining of advantages of both techniques can be possible (3-8). 3D VR technique might change the treatment by showing displacement way in complex fractures. The most of the ortopedist are familiar the X-ray graphies in detection of bone fractures and 3D VR images like the X-ray graphies. As a result, 3D VR images are preferred imaging methods by ortopedists in detection of bone fractures especially in complex anatomic areas in our hospital. Surgical treatment procedures were changed by means of showing exact extension of bone fracture on 3D VR images in three patients with complex bone fractures at shoulder and acetabulum. Fractures of the scapula are often extremely subtle on plain radiographs, but volume-rendered spiral CT is extremely sensitive in the detection and characterization of such fractures. Volume-rendered spiral CT can demonstrate these injuries and display the relevant anatomy in this complex region. CT is often markedly limited secondary to extensive streak artefact from implanted hardware and MR imaging is limited by susceptibility artefact. Spiral CT with volume rendering is often able to compensate for streak artefact, and studies are usually quite successful despite the presence of metal plates, pins, or prostheses (9). For this reason, volume-rendered spiral CT has become preferable modality of choice for postoperative cross-sectional imaging in orthopedic patients Surface and VR techniques can be used in imaging of musculoskeletal pathologies as a 3 D reformatted images. Surface rendering has some advantages. Surface-rendering algorithms can operate very rapidly on modern workstations. The realistic lighting models used in many surface-rendering algorithms can provide the most three-dimensionally intuitive skeletal images. Finally, the distinct surfaces in surface reconstructions facilitate clinical measurements.Two serious drawbacks are associated with the use of surface rendering for the display of skeletal pathology. Most fundamentally, surface renderings depict only the bone surface. Most of the available data is not incorporated into the 3-D image. In cases where the pathology of interest is subcortical or obscured by overlying bone, surface rendering does not display the most important information in the dataset. The second serious drawback is poor image fidelity. Volume rendering has two principal advantages over surface rendering. First, percentage classification provides a physically realistic depiction of volume-averaged CT data. Second, volume rendering incorporates all of the data contained in the volume into the displayed image. Volume renderings can show multiple overlying and internal features, and the displayed intensity is related to the amount of bone encountered along a line extending through the volume (10). As mentioned above, we preferred the VR over the surface rendering in our study. Iodinated contrast material is sometimes necessary for defining the extent of disease and associated abnormalities. Abnormal muscle generally enhances less than normal muscle, and the disease process is thereby accentuated. Definition of the vascular anatomy and soft tissue is also possible by use of contrast material (10). As a conclusion, VR images have become a valuable part of our evaluation of musculoskeletal disease, and we find that their inclusion in our routine musculoskeletal protocols changes management in a significant number of cases. In trauma cases, subtle and complex fractures are better seen on VR images, and complicated spatial information about the relative positions of fracture fragments can be easily demonstrated to the orthopedic surgeons. Postoperative studies in patients with orthopedic hardware also benefit from VR imaging. Spiral CT with VR eliminates most streak artefact and produces high-quality images on which the relationships between hardware, bones, and bone fragments are well demonstrated. REFERENCES
Copyright 2004 - Medical Investigations Society |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}