 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 4, 2004, pp. 65-67 CASE REPORT HYPOTHYROIDISM ASSOCIATED TO MAYER-ROKITANSKY-KUSTER-HAUSER SYNDROME IN A 21-YEAR OLD PATIENT WITH PRIMARY AMENORRHEA Aydın Kurt, Neslihan Gültaşlı, Kemal Rıdvan Yazıcıoğlu, Ali İpek, Gülçin Dilmen, İsmet Taş Ministry of Health Ankara Atatürk Education and Research Hospital, Department
of Radiology
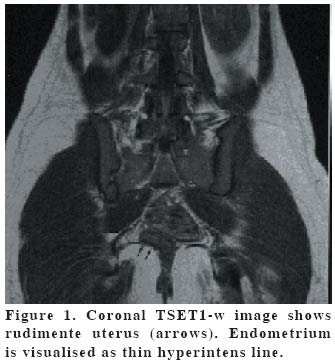
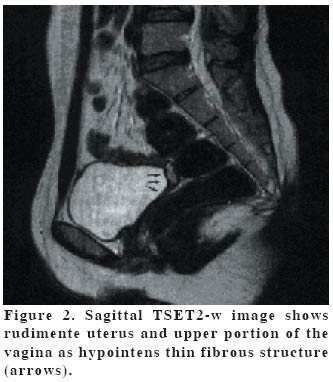
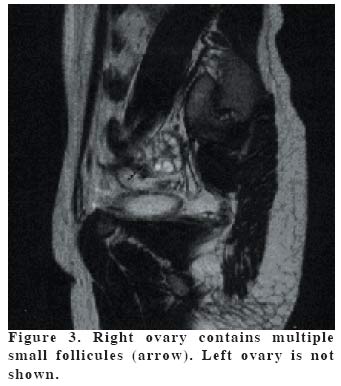
Code Number: gm04046 MRKH syndrome is a rare but widely discussed developmental failure of in part or whole of the Mullerian duct. Twenty-one years old female patient presented with primary amenorrhea and with the history of long-standing hypothyroidism is discussed in this report. INTRODUCTIONMRKH syndrome is a rare but widely discussed developmental failure of in part or whole of the Mullerian duct. The MRKH syndrome occurs in 1 of 4000-5000 female births. Its occurrence with genitourinary and skeletal malformations are common. Its association with endocrine anomalies is very rare (1). Both hypothyroidism and MRKH syndrome cause amenorrhea but their occurrence in the same patient hasn't been reported yet to our knowledge. CASE REPORTTwenty-one years old female patient presented with primary amenorrhea and with the history of long-standing hypothyroidism. She had been treated for hypothyroidism which thought to be the cause of her primary amenorrhea for several years ago. Then she had stopped the medication when the therapy failed. She was 1.52 m tall and weighted 42 kg. No skeletal abnormalities were found. She had normal bone maturation. Normal mental development was observed. In the physical examination ; axillary and pubic hair were scarce, development of breasts was in stage II-III of Tanner. While she had no prior detailed gynecologic examination she was consulted for gynecologic evaluation. Pelvic examination revealed normal external genitalia but small vaginal pouch. Her labaratory tests showed subclinic hypothyroidism. TSH; 7.55 (<10) µU/ml, free T3; 3.17 (70-190) ng/dl, free T4; 0.8 (2.4-6.8) ng/dl, Prolactine; 11 (5-40) ng/ml , FSH; 1.7 (5-30) mIU/ml , LH; 6.7 (522) mIU/ml, progesteron; 5.8 (0-21) ng/ml, estradiol; 2.7 (0-14)µg/ml, cortisol;16 (525) µg/dl. Her FSH level was low which was probably due to the ovarian hypofunction. Her thyroid ultrasound (US)examination was normal. Then she was taken to pelvic US examination. US (Hitachi EUB 6000) revealed the absence of uterus, but a small remnant was suspected. Bilateral ovaries were present and normal. According to the US findings MRKH was suspected and Magnetic Resonance Imaging (MRI) examination was performed to confirm the diagnosis. Coronal TSET1-weighted (w) (TR: 530, TE: 14, slice thickness: 4mm) and sagittal T2-w (TR: 3500, TE: 90, slice thickness: 4mm) images were obtained. MRI (1,5 T, Philips Intera) showed rudimentary uterus (Figure 1-2) and bilateral normal ovaries. Upper portion of the vagina was also rudimentary (Figure 3). These findings revealed the final diagnosis of MRKH syndrome. No other anomalies were found in our patient which reported to be high in MRKH patients. DISCUSSIONPrimary amenorrhea is defined as the failure of menses to appear initially. Wide range of diseases are known to cause primary amenorrhea (1). Diagnosis of the MRKH patients is usually delayed until adolescence. Primary amenorrhea is the reason that leads the patients to the clinician. The main feature of this syndrome is the failure of development of the lower end of the Mullerian duct with the normal growth and development of the secondary sex characteristics. This results in absence of uterus, tubes, cervix uteri and usually the whole vagina. The range of associated abnormalities depends upon the degree of development of the middle and upper thirds of the duct and the Wolfian duct. Approximately one-third of patients with MRKH have renal tract abnormalities, including ectopic kidney, renal agenesis, horseshoe kidney and abnormal collecting tract. Skeletal anomalies are found in %10 to %12 of cases; spine anomalies are common (2, 3, 4). Hypothyroidism is another cause of primary amenorrhea. Sexual development and reproductive function is affected by the thyroid hormones. FSH and LH levels do not usually reach to the levels that suffice the ovulation in the patients with hypothyroidism. Myxedema is the clinical presentation of hypothyroidism. But some patients as in our case who appear clinically euthyroid display labaratory evidence of subclinical hypothyroidism (5). In our case a history of long standing hypothyroidism was present. Her thyroid hormone levels were decreased. Her FSH and LH levels were also low for ovulation as expected in hypothyroidism. She didn't have the classic clinical findings of hypothyroidism and she also had the normal development of secondary sex characteristics that should have led the physicians to suspect the other causes of primary amenorrhea. Through gynecologic and radiologic examination is important for the correct diagnosis and surgery planning of MRKH patients. US is the first method of choice for the diagnosis. In the majority of patients US findings lead the correct diagnosis. But MR examination is also vital to assess the possible associated anomalies. For the correct surgery planning MR has taken the place of laparoscopy (6). REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04046f3.jpg] [gm04046f1.jpg] [gm04046f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}