 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 1, No. 4, 2004, pp. 74-77 CASE REPORT ORBITAL EXTENSION OF A LARGE FRONTAL SINUS OSTEOMA ASSOCIATED WITH FIBROUS DYSPLASIA Aylin Yücel, Murat Acar, Alpay Haktanır, Ramazan Albayrak,Bumin Değirmenci Afyon Kocatepe University, Faculty of Medicine, Department
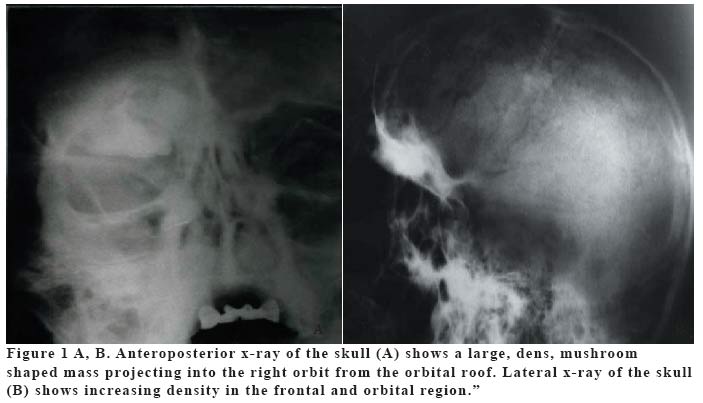
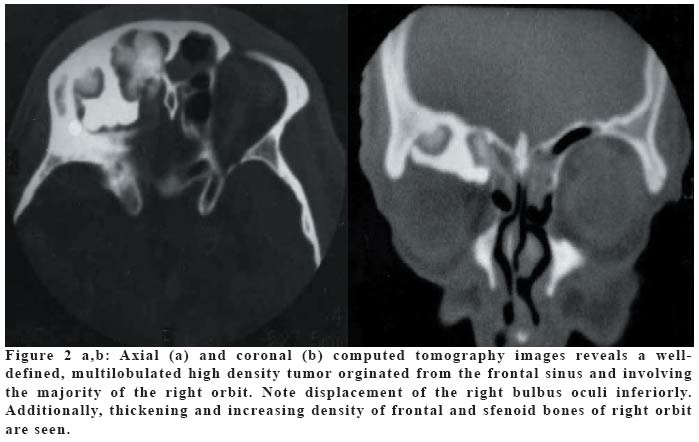
of Radiology Code Number: gm04049 Osteoma is the most common benign tumor of the paranasal sinuses that is capable of extending to surrounding structures. Fibrous dysplasia is a benign developmental abnormality of the bone with unknown etiology. We describe a patient with osteoma of the frontal sinus who presented with right proptosis. And also fibrous dysplasia of skull adjacent the osteoma was found incidentally. Key words: Osteoma, fibrous dysplasia of bone, frontal sinus, orbit. INTRODUCTION Osteoma is the most common benign tumor of the nose and paranasal sinuses, and the frontal sinus is its more frequent location (1,2). Paranasal sinus osteoma is a slow-growing, encapsulated bony tumor that may be commonly asymptomatic, being detected incidentally in 1% of plain sinus radiographs or in 3% of sinus computerized tomographic scans (3). Osteomas are a frequent cause of mucoceles and sinusitis due to blokage of the nasal ducts, but they can also present with more dramatic signs, such as orbital or intracranial invasion (4,5). If larger and invading the orbit, they result in proptosis and/or globe displacement and ocular motility problems (3,5). Fibrous dysplasia is a benign proliferation of fibrous tissue and woven bone (5). This is a disease of unknown etiology and usually found incidentally or following pathological fracture (6). We describe a patient with osteoma of the frontal sinus who presented with right proptosis and severe periorbital swelling. And also fibrous dysplasia of skull adjacent the osteoma was found incidentally. To the best of our knowledge, this is the first case has been presented osteoma associated with fibrous dysplasia of the orbit. CASE A 49 year-old man presented with severe periorbital swelling. At physical examination, inferior lateral displacement of the right eye ball, superior lateral limitation of right ocular motility and proptosis were detected. Fundoscopic examination revealed no papilledema or evidence of optic atrophy. Anteroposterior x-ray of the skull showed a large, dense, mushroom shaped mass projecting into the right orbit from the orbital roof (Figure 1a). Lateral x-ray of the skull showed increasing density in the frontal and orbital regions (Figure 1b). Axial and coronal computed tomography images revealed a 3.5x3x4 cm well-defined, multilobulated high density tumor, orginated from the superior wall of the frontal sinus and involving the majority of the anterior superior right orbital region. Extension into the orbit with narrow neck was noted. The mass had displaced the right superior rectus muscule and bulbus oculi inferiorly. (Figure 2a,b). Asymetrical thinning of the right optic nerve and increasing calibration of the right superior ophthalmic vein were markedly apparent. In addition, thickening and increasing density like "ground glass"of frontal and sfenoid bones of right orbit were seen in these images. On the basis of the x-ray and CT findings, the diagnosis of a large osteoma of the frontal sinus associated with fibrous dysplasia of frontal and sfenoid bones was made. After diagnosis, patient underwent surgical operation. Postoperatively, eye movements returned to normal and proptosis progressively decreased. Now, four year after the operation, the patient is symptom-free, with no tumor recurrence and no progression of fibrous dysplasia. DISCUSSION Symptoms referable to frontal sinus osteomas are variable and usually proportional to the size of the tumor. Many small osteomas are asymptomatic (2). A progressively enlarging osteoma can, although rarely, outgrow the sinus walls causing forehead deformity, intraorbital or intracranial complications (7). The etiology of osteomas is controversial. The most accepted theories are embryologic, traumatic or infectious causes (2,5). In favor of the developmental theory is the fact that many osteomas appear to rise at the junction of the ethmoid and frontal sinuses, a location where membranous and cartilaginous tissues meet during embryonic life (3). Trauma during puberty, when bone development is at its maximum, has been implicated in several cases of osteoma (3). Sinusitis may stimulate osteoblastic proliferation within the mucoperiosteal lining of sinuses that cause tumor formation (3,8). Despite the coexistence of sinusitis with osteoma, some authors believe that the sinusitis results from occlusion of sinus opennings by the osteoma (3). The occurence of osteomas in the setting of Gardner's Syndrome (assosiated with soft tissue tumors and high-risk intestinal polyps) must be kept in mind (7). Osteomas generally become symptomatic in the second to fifth decades of life (8). The ratio of males to females about 2 to 1 (2). The greater preponderance of sinus osteomas in man is attributed to man's greater exposure to trauma and the larger size of their sinuses (3). Clinical onset is most often characterized by facial pain and headache, while a predominantly intraorbital growth leads to proptosis, diplopia and amaurosis fugax (7). On the other hand, some intracranial complications may occur as a result of extensive destruction of the anterior cranial fossa; they include pneumatocele, mucocele, abscess formation, meningitis and cerebrospinal fluid rhinorrhea (9). Since its first use in the diagnosis of osteomas in 1899, radiography has become the method of choice for diagnosis of osseous lesions (3). Osteomas are easily demonstrated by plain radiographs, CT or magnetic resonance imaging (MRI) as localized, isolated, markedly radiodense lesions resting on the floor of the sinus and expanding the involved sinus with or without orbital or intracranial extension (3). These findings usually consent to differentiate osteomas from other bone tumors, and from fibrous dysplasia (9). Spiral CT helps to give a three-dimensional reconstruction of the tumor (3). MRI is important in the definition of dural or soft tissue involvement. The orbital extensions are well defined in the coronal and sagittal images; which provide a good evaluation of the roof of the orbit. The relationship of the tumor with the optic canal and optic nerve is well shown in axial sections (9). Radionuclide bone scan can help to differentiate an actively growing lesion ("hot") from a stable lesion ("cold"). Orbital venography has been used to demonstrate compression of the superior ophthalmic vein (3). No treatment recommended for asymptomatic osteomas, especially in elderly patients. They can be followed radiographically (5,8,10). If significant growth or clinical sign is shown, a more aggressive posture could be used (10). The type of procedure selected depends on the location and extent of the osteomas and the nature of any existing complications (11). In the orbital region, anterior lesions can be removed via an anterior orbitotomy, while more posterior tumors require an orbitocranial procedure (5). Our case had severe proptosis, and after operation, proptosis and eye movements returned to normal. Recurrence of these tumors is rare (5), and there was no recurrence in our case during a follow up period of four years. Fibrous dysplasia has been described in three forms: monostotic, polyostotic, and McCune-Albright syndrome (5). In the skull, a grossly expansile, sclerotic lesions are seen. Lesions do not really need to be diagnosed by biopsy, as the appearances are usually characteristic (6). Localized thickening of calvarium with expansile sclerotic lesion was also seen in our case. The majority of cases with orbital involvement have monostotic fibrous dysplasia, with the frontal bone followed by the sfenoid and ethmoid being most commonly affected (5). In our case, frontal and sfenoid bones were affected. The disease has a roughly equal sex distribution (5). The age of onset is usually between 10 and 30, but can present late in adult life (5,6). Prognosis is worse when the lesions occur early in life (6). Long-standing facial asymmetry, proptosis, and globe displacement are common presentations. Cranial nerve palsies, raised intracranial pressure, and nasolacrimal duct and nasal obstruction can also occur (5). Our case was adult and he was followed up during four years and there was no symptomatic progression in the disease. In conclusion, frontal sinus osteomas can cause proptosis with orbital extension. It must be kept in mind for differential diagnosis of proptosis. Osteoma associated with fibrous dysplasia have not been described previously. Both of them has unknown etiology and originated from benign proliferation of bony tissue. The coincidence in our case can be explained by similiar etiologies. REFERENCES
Copyright 2004 - Medical Investigations Society The following images related to this document are available:Photo images[gm04049f2.jpg] [gm04049f1.jpg] |
| |||||||||

{kind=link}
{kind=link}