 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 1, 2005, pp. 5-9 ORTHOSTATIC HYPOTENSION AND HEART RATE VARIABILITY AS INDICATORS OF CARDIAC AUTONOMIC NEUROPATHY IN DIABETES MELLITUS Abdülkadir Koçer1, Zekeriya Aktürk2, Emin Maden3, Atilla Taşçı4 1PTT Training and Research Hospital, Departments of Neurology1 and
Internal Medicine4, İstanbul, Trakya University Medical Faculty,
Department of Family Medicine2, Edirne, Sureyyapasa Chest Diseases
and Thoracic Surgery Training Hospital3, İstanbul, Turkey Code Number: gm05002 Aim: The aim of this study was to emphasize
two different points in our work: 1) The well known importance of (subclinical)
postural hypotension and reduced heart rate variability as (early) markers
of autonomic neuropathy; 2) and the more controversial influence of diabetic
control in their worsening. Key words: Diabetes, autonomic neuropathy, HbA1c, QT interval, heart rate variability, orthostatic hypotension INTRODUCTION Autonomic neuropathy is a common problem in diabetics (1-3). The most important sign of diabetic autonomic neuropathy (DAN) is QT interval prolongation, one of the causes of sudden death in diabetic patients. Other diabetic complications are also frequently seen in DAN patients. Disturbances of heart rate related to respiration and orthosthatic hypotension are the most commonly seen manifestations of cardiovascular neuropathies in diabetics. Although deaths in diabetic patients are generally related to macrovascular diseases, cardiac autonomic neuropathy decrease the survival by 20 percent (2,3). Cardiac autonomic neuropathy is an important complication that occurs with time in every diabetic. The incidence of cardiac autonomic neuropathy rises parallel with the known duration of diabetes. Studies have found a positive correlation between the findings of cardiac autonomic neuropathy and the known duration of diabetes (4,5). Hemoglobin A1c (HbA1c) is the parameter most commonly used for the quantitative determination of glycemic control and the maintenance of low levels of blood HbA1c, which is an important criterion for diabetic control. HbA1c is inversely related to the development of complications (6). The measurement of QT interval is suggested as a sensitive, non-invasive, and simple predictor of cardiac dysautonomia (7). QTc has not been widely used to assess autonomic function, even though it is easier to measure than performing HRV testing, and we do not know the association of BP and HRV with prolonged QTc. We hypothesized that postural blood pressure changes and respiratory changes can be used as clinical indicators of cardiac autonomic neuropathy. Hence, we designed a study to assess the importance of postural blood pressure changes and respiratory changes in heart rate as cardiovascular signs of autonomic neuropathy (4). The aim of this study was to evaluate the importance of the clinical indicators of postural blood pressure changes and respiratory changes in heart rate as cardiovascular signs of autonomic neuropathy. MATERIAL AND METHOD This study was conducted on 93 diabetic patients (50 males (53.8 %), 43 females (46.2 %)). 17 of the patients were receiving insulin whereas the remaining 76 were on oral anti diabetics. The inclusion criteria were defined as 1- established diagnosis of diabetes according to the American Diabetes Association criteria, 2- A QTc value of above 0.5 seconds, and 3- the absence of any drug usage. Exclusion criteria were 1- the presence of any accompanying disease and 2-the presence of any cardiac rhythm abnormalities. All subjects included in this study had undergone a detailed physical and cardiovascular examination to disclose any concomitant disease, drug usage, and cardiac rhythm abnormalities, which could lead to QT prolongation. Investigators, performing the measurements were blinded to the symptoms, duration, and control of diabetes. Two standard cardiovascular response tests were carried out to determine cardiac dysautonomy: the variation of heart rates in respiratory cycle and the drop in systolic blood pressure on standing (postural hypotension). The variation of heart rates in inspiration and expiration (i.e. beat-to-beat heart rate test) was determined electrocardiographically. The patients were positioned supine (head elevated up to 30 degree) and asked to make inspiration for 5 seconds then expiration for 5 seconds. This was repeated six times. The longest (minimal heart rate) and shortest (maximal heart rate) R-R intervals on electrocardiography (ECG), and heart rate variation (maximal heart rate - minimal heart rate) were determined. The variation of heart rate during inspiration and expiration of less than 20 beats per minute is accepted as autonomic dysfunction (8). Supine blood pressures after 10 minutes of rest were measured. Then, blood pressure measurement was repeated after 3 minutes of active standing with handgrip. Differences in systolic blood pressure while in standing and supine positions were calculated (5). The variation of heart rate related to respiration does not influence QT interval. Therefore, QT interval was measured on an ECG recorded at rest and corrected for the cardiac cycle length (QTc). QTc was calculated by the equation of Bazett:
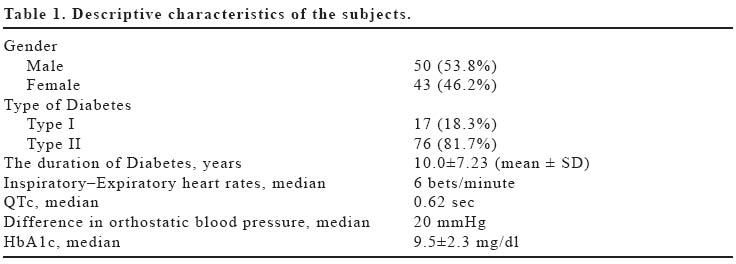
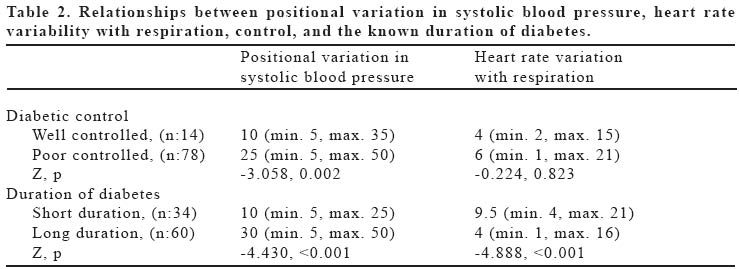
We used QT elongation as a marker of cardiac autonomic neuropathy. Blood glucose and HbA1c levels were analyzed. Patients with HbA1c<7 were considered as well-controlled diabetics. The relations between DAN findings and diabetic control were determined. Two groups were defined depending on the known duration of diabetes (i.e.>5 and <5 years). The relationship of postural changes in blood pressure and heart rate variability with respiration to the duration as well as control of diabetes were evaluated. Patients were divided into subgroups according to diabetic control [well controlled (n:14) vs. poor controlled (n:78)] and diabetes duration [short duration (n:34) vs. long duration (n:60)] and evaluated for the presence of clinical cardiac autonomic neuropathy indicators. The dependent variables in the analysis were "difference in orthostatic blood pressure", "QTc", "heart rate variation with respiration", and "positional variation in systolic blood pressure". Independent variables were "sex", "type of diabetes", "average known duration of diabetes", and "diabetes control (HbA1c)". Continuous variables were tested for normal distribution using the Kolmogorov-Smirnov test, which revealed that none of the dependent variables had normal distribution. Hence, statistical analysis was done with Mann-Whitney U test and Spearman correlation. RESULTS Descriptive data of the study population are shown in Table 1. The median age of the patients was 62 years (min: 32, max: 76). Thirty four patients had diabetes for equal or less than 5 years while 59 patients had diabetes for more than 5 years. Seventy six patients were using oral anti diabetic medications whereas 17 patients were on insulin therapy. All cases had QTc prolongation (min.: 0.505, max.: 0.896, median: 0.620). Fourteen patients (15.2%) had well-controlled diabetes whereas 78 patients (84.8%) had poor controlled diabetes. Median QTc intervals were 0.604 (min. 0.505, max. 0.890) and 0.625 (min. 0.510, max. 1.986) for males and females respectively. There was no statistically significant relationship between categorized QTc values and gender of the patients (Z: -0.470, p:0.633). The comparisons of median positional blood pressure differences and heart rate variability with regard to diabetic control and the known duration of diabetes are presented in Table 2. Manifestations related to cardiac autonomic neuropathy were more prominent in cases whose known duration of diabetes was > 5 years, when compared with patients who were diabetics for < 5 years. Postural blood pressure differences increased while the heart rate variability decreased with the duration of diabetes. Blood pressure variations with standing were significantly related with the control (t:-3.089, p:0.003) as well as the duration of diabetes (t:-5.576, p<0.001). Variability of hearth rate with respiration on the other hand, was significantly related to the duration (t:5.045, p<0.001) but not to the control (t:0.044, p:0.965) of diabetes. QTc showed a significant correlation with the duration of diabetes, postural blood pressure changes, and heart rate variability with respiration (Spearman R, p (0.552, <0.001), (0.258, 0.012), and (-0.488, <0.001) respectively). DISCUSSION The prolongation of QTc interval is a characteristic of cardiac autonomic neuropathy (1,9,10). The clinical significance of QTc prolongation is determined by its frequency, length and its association with adverse clinical events. Previous studies have shown significant correlations between QTc prolongation and autonomic cardiac dysfunction. QTc prolongation is predictive of increased mortality and decreased survival with ventricular arrhythmias in diabetic patients (11). Abnormal QTc interval is an indicator of sympathetic and parasympathetic nervous system dysfunction (7,12). Although a controversy exists relating to the upper limit of normal of QTc interval, a QT interval over 0.5 seconds definitely necessitates an urgent intervention such as a cardiac evaluation or revision of the treatment (13). Since all cases in this study had QTc values above 0.5 seconds, it is clear that we deal with a population having serious cardiac autonomic neuropathy. We found patients with neuropathy induced QTc prolongation up to 0.89 seconds with a median QTc of 0.62. This was astonishing as we know that the mean neuropathy induced QTc prolongation was less than 0.50 seconds in most studies (7,11,12,13). Although it is relatively easy and quick to measure QTc levels, other signs supporting this serious diagnosis will be useful as well. Orthostatic hypotension or induction of hypotension with exercise are cardiovascular neuropathic manifestations of diabetes which primarily are the result of afferent sympathetic vasomotor degeneration. Postural hypotension is frequently observed and interpreted as a hypoglycemic reaction (14,15). The fact that positional changes in systolic blood pressure are significantly affected by the duration and control of diabetes, and at the same time show high correlation with the QTc values, increases the importance of this sign in the evaluation of cardiac autonomic neuropathy. Under normal conditions, the heart beats in a predetermined rhythm. Generally, sympathetic stimulation enhances and parasympathetic stimulation reduces cardiac contractility. The number of heart beats per minute ranges between 20-30 beats/min and 150-250 beats/min under maximal vagal and sympathetic influences. Because of involvement of cardiac autonomic nerves, heart rate increases in diabetic patients compared with their healthy peers (8). Vagal degeneration causes respiratory changes in heart rates and leads to tachycardia. In our study, beat-to-beat variations in heart rates related to respiration have been assessed. Heart rate variability too seems to be an important predictor of cardiac autonomic neuropathy, but this finding should probably be evaluated more cautiously since it is not affected from the control of diabetes. DAN characterized by alteration of small nerve fibers presents with both sympathetic and parasympathetic problems. Diabetic cardiac autonomic neuropathy is an important clinical entity affecting both parasympathetic (tachycardia at rest, change in the heart rate during deep inspiration) and sympathetic systems. Parasympathetic involvement is more frequent and can appear during the early stages of diabetes. Available information shows that this type of neuropathy shortens survival, enhances the risk of ventricular arrhytmia and accelerates sudden death. The rising incidence of Q-T prolongation at rest and after exercise supports this hypothesis (10). While diabetes duration was associated both with heart rate variations with respiration and positional variation in systolic blood pressure, diabetic control was only associated with heart rate variations with respiration. In fact, there are factors other than HbA1c in the prognosis of diabetes and it seems that the duration of diabetes is a stronger predictor than diabetic control in the prognosis of diabetes. In our study, manifestations related to cardiac autonomic neuropathy were more prominent in cases whose known duration of diabetes were > 5 years, when compared with patients who were diabetics for 5 years or less. Hence, we suggest checking orthostatic hypotension and heart rate variability in all patients with a diabetes history of five years or more. In conclusion, this analytical study confirmed the importance of the clinical variables 'heart rate variability by respiration' and 'orthostatic blood pressure changes'in diabetic patients with cardiac autonomic neuropathy. Health professionals caring for diabetic patients should be more alert for the signs of autonomic neuropathy, especially in patients with a history of diabetes for more than five years. Special attention should be given to postural blood pressure changes and heart rate variability with respiration together with QT interval elongations. However, further studies involving health persons and diabetic patients with normal should be performed in order to reveal the real value of the mentioned clinical indicators in diabetic autonomic cardiac neuropathy. REFERENCES
|

{kind=link}
{kind=link}