 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 1, 2005, pp. 14-19 EPIDEMIOLOGY OF SELF-IMMOLATION IN THE NORTH-WEST OF IRAN
Dastgiri S1, Kalankesh LR2, Pourafkary N3 Tabriz University of Medical Sciences, Department of Epidemiology and Public Health ,and National Public Health Management
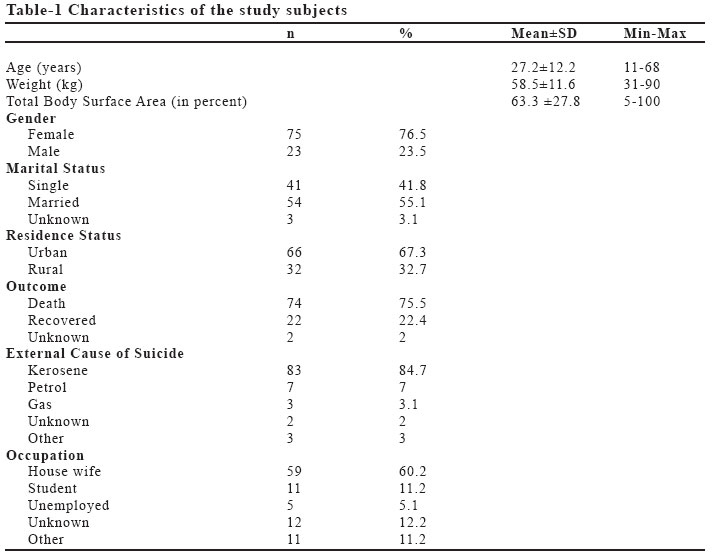
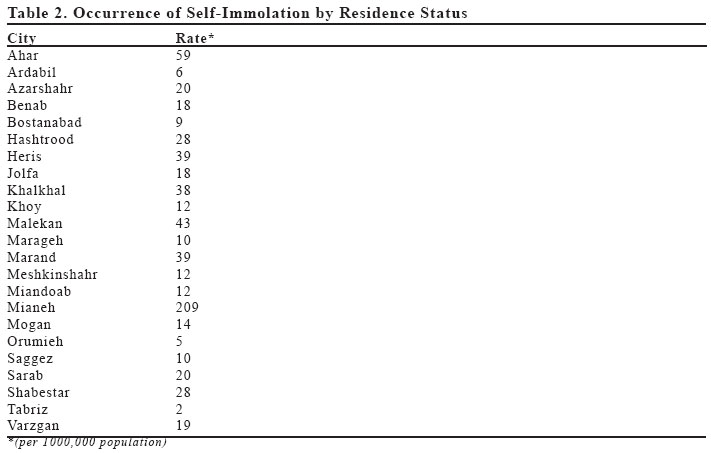
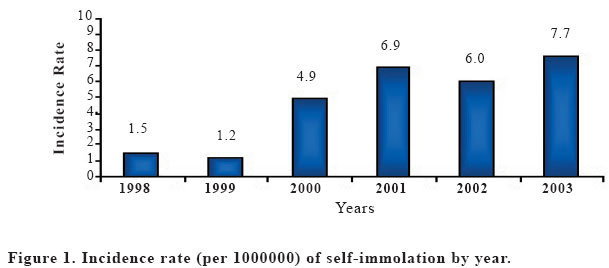
Centre (NPMC)1, Department of Medical Records2 and Department of Psychiatry3, Tabriz, Iran Code Number: gm05004 Aim: This study was carried out to investigate the incidence, time trend, influencing factors and survival of self-immolation in the North-West of Iran.Methods: In this research, medical records of ninety eight cases who attempted suicide by self-immolation between 1998 and 2003 were studied. Data collected included age, weight, sex, marital status, date of burn, length of stay in the hospital, body surface burned (in percent), external cause of death, psychiatric diagnosis of patients, and outcome. Incidence rates and descriptive statistics were calculated to document the epidemiological features of the self-immolation in the region. Survival rates with 95% confidence intervals were calculated using the Kaplan-Meier method to assess the survival pattern of the suicide by self-immolation. Results: The mean age of subjects was 27 years (range: 11-68 years). The female / male ratio was 3.3. Most of the cases were married (55 percent). There was an increasing trend in the incidence rate of self-immolation from 1998 (1.48 per 1000,000 population, CI95%: 0.2-2.8) to 2003 (7.7 per 1000,000 population, CI95%: 4.8-10.5). Two and five weeks survival rates for suicide by self-immolation were 25 percent (CI 95%: 16-34) and 15 (CI 95%: 6-24), respectively. Conclusion: Availability of family mental health centers, easy access to emergency services, and psycho-educational programmes to high-risk groups (i.e. young women) may reduce the increasing rate of self-immolation in the region. Key words: Epidemiology, Self-immolation, Iran INTRODUCTION Suicide, an act in which individuals sacrifice voluntarily themselves, is considered as a serious psychosocial problem. Of all forms of suicidal attempts, self-immolation is perhaps the most dramatic, violent and often the most difficult to understand one (1). While suicide by self-immolation is very rare in developed world, it is more frequent in some other countries (i.e. Africa, Middle East, Far East, Egypt, India, and Vietnam) where it is somehow linked to religious believes (2-5). Sheth and colleagues reported that self-immolation, in India for instance, accounts for up to 40 percent of suicides (4). Some reports show that the proportional frequency of self-immolation is about 25-40% of all forms of suicides in Iran. It is the second (after hanging) cause of death among completed suicides (6,7). This study was carried out to investigate the incidence, causes, influencing factors, and prognosis of self-immolation in North-West of Iran. MATERIAL AND METHODS In this research, medical history of ninety-eight cases that committed suicide by self-immolation between 1998 and 2003 in North West of Iran, were studied. All subjects were prospectively followed since psychiatric diagnosis and admission at hospital to assess the outcome of suicide. Data collected included age, weight, gender, marital status, occupation, date of burn, length of stay in the hospital, treatment, residence status, Total Burn Surface Area (TBSA- in percent), external cause of death, psychiatric diagnosis of patients, and outcome. Incidence rates and descriptive statistics were calculated to document the epidemiological features of the self-immolation in the region. Survival rates with 95% confidence intervals were calculated using the Kaplan-Meier method to assess the prognosis of the suicide by self-immolation. RESULTS Between1998 and 2003, Ninety eight cases of attempted suicide by self-immolation were diagnosed and ascertained in Sina university-hospital of Tabriz University of Medical Sciences, Tabriz, Iran. Table-1 shows the basic characteristics of the study subjects. The mean age (Standard Deviation) of cases was 27 (12) years (range: 11-68 years). The female / male ratio was 3.3. Majority of the cases were married (55%). Kerosene was the most common tool (85%) used to commit suicide by self-immolation. The average burn size was 63 percent of total body surface. Case fatality rate was 76 percent. Twenty eight and fifteen percent of cases had a history of family conflicts and mental disorders, respectively. Table 2 shows the incidence rate of self-immolation by city of residence in the North-West of Iran. The lowest and highest incidence rate (per 1000,000 population) of self-immolation occurred in Tabriz (2, CI 95%: 1.2-2.8) and Mianeh (209, CI 95%: 72.5-346), respectively. There was a significant increasing trend in the incidence rate (per 1000,000 population) of self-immolation from 1998 (1.48, CI 95%: 0.2-2.8) to 2003 (7.7, CI 95%: 4.8-10.5) (Figure 1). The majority of suicides by self-immolation occurred in March every year (Figure 2). Figure 3 shows the survival pattern in attempted suicides by self-immolation. Two and five weeks survival rates for suicide by self-immolation were 25 percent (CI 95%: 16-34) and 15 (CI 95%: 6-24), respectively. The median survival time was 4.3 days (CI 95%: 3.9-4.5). DISCUSSION Most the cases committing suicide usually use nonviolent methods in many countries. There are, however, considerable differences between eastern and western societies in terms of the methods used for suicide. Self-immolation is a suicidal method happening frequently in a number of countries (6). The reasons for self-immolation vary by different countries ranging from socio-economic issues to political protests (8). In our study self-immolation incidence rate has increased in 2003 compared to 1998. Some previous studies have shown that incidence of self-immolation has risen by 30-40 percent in Kermanshah and Ilam provinces of Iran over the past few years (9). Some researches have reported the self-immolation as one of the most common methods of suicide in Iran (6,7,10). The mean age of self-immolation victims in Iran is relatively low compared to western countries. Some studies have shown that the mean age of victims in Iran ranging between 18-27 years (6,11,12) which is almost similar to the findings of present study, while the same figures from industrial countries have been reported between 38-43 years (13-15). It may therefore be concluded that influencing factors in developed countries are different of those in the less developed countries. The main reasons in less developed countries seem to be socio-economic factors while in developed countries it may happen as a political protest only. For instance, deprivation, poverty and humiliation in Uzbekistan; problems related to marriage and trousseau in India; and forced marriage in Afghanistan have been reported as the main factors of self-immolation in young women (16-18). There was almost a similar finding in our study where the incidence of self-immolation in most deprived cities was higher than affluent ones. Our study indicated that the occurrence of self-immolation among females is much higher than males. This difference between females and males is similar to the research data reported from the provinces of Mazandaran, Ahvaz, and Kordistan in the country (6,12,11). The same gender difference has also been reported from Egypt, Zimbabwe, Serilanka, India, Afghanistan and Uzbekistan (16,19-25). In contrast, studies from European countries, Australia and North America have shown that men committing suicide by self-immolation more than women (26,27). According to Cameron et al. in a study from Australia, all of the cases committed self-immolation were almost male (26). Fifty five percent of our subjects in this study were married. Similar findings have been reported from other parts of the country (6,12,28) indicating that family conflicts might have had a remarkable role in self-immolation occurrence as a causal factor. Different kinds of mental disorders and drug abuse have been reported in different studies as an important factor causing self-immolation. In our study, fifteen percent of cases had a clinical history of mental disorder. Much higher figures have been reported from Turkey (83%), Finland (87%), Egypt (30%) and Germany (33%) (8,13,19,29-31). Seventy five percent of cases in our study died during the first two weeks. According to the research data from India, Germany, Turkey, Finland and Japan, the burn surface has had a key impact on the mortality of subjects after committing suicide (8,13,23,29,30) where the more the burn surface, the more the mortality rate. Easy access to health and medical clinics, and availability of emergency services for cases committed self-immolation may avoid burn surface to become wider reducing the probability of mortality in patients. We conclude that as easy access to inflammable materials may have an important role in committing suicide by self-immolation, it is therefore recommended that the access to such materials should be limited in high-risk people. Further more, availability of family mental health centers, easy access to emergency services, and psycho-educational programmes to high-risk groups (i.e. young women) may reduce the increasing rate of self-immolation in the region. REFERENCES
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}