 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
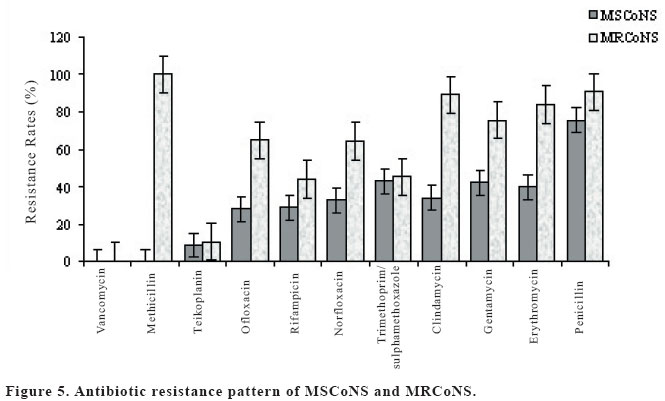
European Journal of General Medicine, Vol. 2, No. 1, 2005, pp. 20-26 PREVALENCE OF METHICILLIN-SENSITIVE AND METHICILLIN-RESISTANT STAPHYLOCOCCI IN INTENSIVE CARE UNITS IN A UNIVERSITY HOSPITAL Lütfü Savaş1, Nizami Duran2, Yusuf Önlen1, Nazan Savaş3,Sabahattin Ocak1, Nur Efe İris4 Mustafa Kemal University, Medical Faculty, Departments of Infectious Diseases
and Clinical Microbiology1, Microbiology2 and
of Public Health3, Hatay. SSK Okmeydanı Hospital4, İstanbul,
Turkey Code Number: gm05005 Aim: The intensive care units (ICUs) are burdened with a high frequency
of nosocomial infections often caused by multiresistant nosocomial pathogens.
Coagulase-negative staphylococci (CoNS) and Staphylococcus aureus are
reported as important causative agents of nosocomial infections. The objective
of this study was to identify frequency of methicillin resistant and susceptible
staphylococci from the various clinical samples in ICUs, and to investigate
resistance patterns against various antibiotics used broadly for treatment.
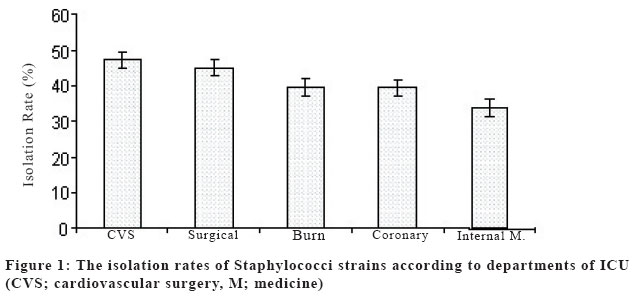
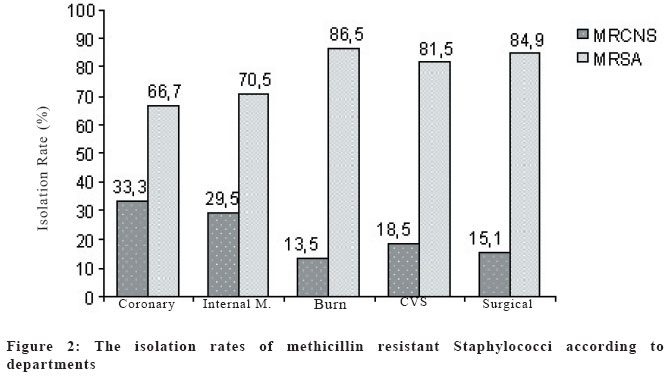
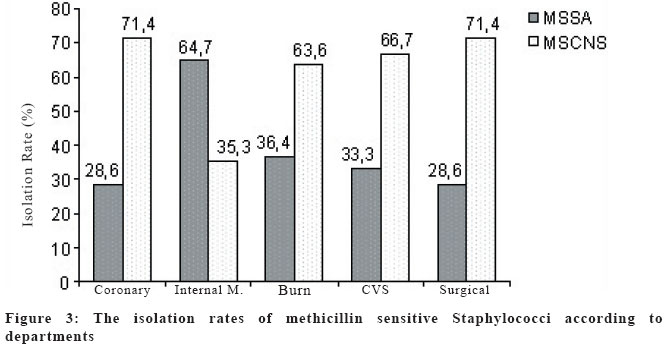
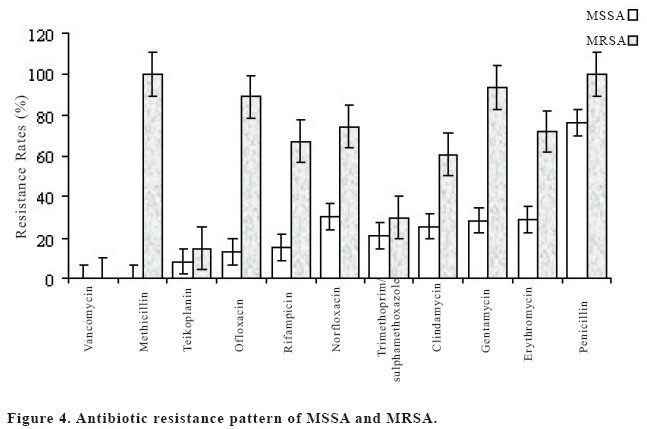
Key words: Staphylococci, MRSA, ICUs, methicillin, susceptibility. INTRODUCTION Patients hospitalised in the intensive care unit (ICU) are at particular risk for acquiring nosocomial infections due to serious underlying diseases, compromised membrane and skin barriers following the use of invasive devices, and extended length of hospital stay are among other factors. Exposure to various antimicrobial agents may further complicate such hospitalizations and create conditions conducive to resistance selection among host bacterial flora or nosocomially-transmitted pathogens. Studies have demonstrated that rates of antimicrobial resistance are greater in bacteria isolated from ICUs compared with other hospital wards and outpatient clinics (1,2). In general, Gram-positive organisms such as Staphylococcus aureus and CoNS are commonly associated with nosocomial infections among ICUs patients. Examination of the rates of antimicrobial resistance among these pathogens shows that rates of MRSA and methicillin-resistant CoNS have increased steadily over the past decade (1,3). Determination of in-vitro resistance of Staphylococcus aureus, which causes hospital originated infection, is curicial to apply an appropriate antibiotics. Especially, methicillin-resistant strains exhibits serious clinical problems. It has been reported that the rate of MRSA has increased significantly after 1980's (4,5). Despite rapid development in antimicrobial treatment, there are still great difficulities in treatment of staphylococcal infections. It has been reported that methicillin-resistant and susceptible staphylacoccci also exhibit resistance to β lactam antibiotics as well as other antibiotics. Since staphylococci may cause hospital epidemics, they are considered as a potentially important health problem in all over the world (6,7,8). Staphylococcci are important hospital pathogens, the incidence of which is increasing every year especially in high risk groups such as ICUs. MRSA is a pathogen of special concern in ICUs. The burn units are very susceptible habitats to colonization and infection events by this organism. MRSA is a major problem in ICUs in most countries (9). This study was undertaken to find out the prevalence of methicillin resistant and sensitive staphylococci in ICUs of our hospital and to compare their antibiotic susceptibility patterns. MATERIALS AND METHODS Microbiological analysis This prospective study was conducted in the ICUs and burn center of a teaching hospital over a period of 6 months. This study was undertaken to find the prevalence of hospital-acquired MRSA infection in Baskent University Hospital in Adana between June 2002-December 2002. In this study, 241 staphylococci were isolated from 597 patients hospitalized in four different ICUs (coronary ICU, surgical ICU, internal ICU, cardiovascular surgical ICU) and burn center. To isolate staphylococci, samples were inoculated onto sheep blood-agar plates and phenol-red mannitol salt agar plates. The plates were incubated at 37 °C for 48 h. All the samples were cultured quantitatively and qualitatively, and strains were identified by colony morphology, by Gram staining, by catalase tests, and by coagulase tests (10). All isolated staphylococci strains were identified using standard procedures and antimicrobial susceptibility testing was performed according to the guidelines of the National Committee for Clinical Laboratory Standards (NCCLS) by using Kirby-Bauer disc diffusion method (11). Strains producing inhibition less than 10 mm zone diameter or producing no inhibition were considered resistant against methicillin. Susceptibility of isolated staphylococci strains against methicillin (10μg/disc), penicillin (10μg/disc), gentamycin (10μg/disc), trimethoprim-sulphamethoxazole (1.25/23.75μg/ml) erythromycin (15μg/disc), rifampin (5μg/disc), clindamycin (2μg/disc), teicoplanin (30μg/disc), ofloxacin (5μg/disc), norfloxacin (10μg/disc), and vancomycin (30 μg/disc) were tested. All antibiotic discs were obtained from Oxoid firm (Oxoid, Hampshire, England). As a control strain, ATCC 25923 was used for identification and susceptibility tests. Statistical analysis Statistical analysis was performed using a chi square test and p values less than 0.05 were considered as statistically significant. The statistical analysis were performed by using Statistical Package for Social Sciences (SPSS, ver 10.0) software. RESULTS In this study, staphylococci were isolated from 241 out of 597 patients (40.4 %) from whom nasal, urinal, throat, blood, and tracheal aspiration samples were taken. MRSA (24.1%, 144/597) and methicillin-sensitive Staphylococcus aureus (MSSA) (9.96%, 24/241) were detected on the isolates. The rates of methicillin-sensitive CoNS (MSCoNS) and MRSA on the isolated samples were 14.5% (35/241) and 15.8% (38/241). Figure 1, 2 and 3 show the departments from which staphylococci were isolated. Of the 241 stophyloccocci strains isolated, 69.7% (168/241) was Staphylococcus aureus and 30.3% (73/241) was CoNS. Methicillin-resistance rate was 85.7% among the Staphylococcus aureus strains while it was 52.1% (38/73) among CoNS (p<0.001). The most effective antibiotics against MSSA, MRSA and CoNS strains were glycopeptides and out of 241 staphylococci strains no resistance was found against vancomycin. However, resistance rates against teicoplanin of MRSA, MSSA, MRCoNS and MSCoNS were 14.7% 8.5%, 10.5% and 8%, respectively. Apart from glycopeptides, most effective antibiotics against MRSA strains were trimethoprim-sulphamethoxazole (29.9%), clindamycin (60.8%), rifampin (67.2%) and erytromycin (71.8%). Also it is determined that ofloxacin (13.1%), rifampin (15.0%) and trimethoprim-sulphamethoxazole were the most effective antibiotics against MSSA. Rifampin (43.7%) and trimethoprim-sulphamethoxazole (45.1%) were found to be the most effective against MRCoNS while ofloxacin (27.9%) and rifampin (28.6%) were the most effective against MSCoNS. DISCUSSION Staphylococci are pathogens of special concern in ICUs. ICUs are very susceptible habitats to colonization and infection events by this organism. Staphylococcus aureus is recognized as one of the most important bacterial pathogens seriously contributing to the problem of hospital infections all over the world. Resistance to multiple antibiotics among the Staphylococcus isolates in hospitals has been recognized as one of the major challenges in hospital infection control (5,8). Nosocomial infections affect about 30% of patients in ICUs and are associated with substantial morbidity and mortality. Management of nosocomial infection relies on adequate and appropriate antibiotic therapy, which should be selected after discussion with infectious diseases specialists and modified when microbiological data become available (12). The incidence of infection in ICUs is one of the highest in the hospital and as yet facilities to prevent infection are often inadequate in this important clinical area. Many antibiotic resistant bacteria such as MRSA, may survive (6). The identification and control of MRSA is of primary concern in ICUs worldwide (13). Patients hospitalized in ICUs are 5 to 10 times more likely to acquire nosocomial infections than other hospitalised patients. The frequency of infections at different anatomic sites and the risk of infection vary by the type of ICU, and the frequency of specific pathogens varies by infection site. Contributing to the seriousness of nosocomial infections, especially in ICUs, is the increasing incidence of infections caused by antibiotic-resistant pathogens (14). Knowledge of the antibiotic susceptibility of the organisms isolated in the ICU helps to formulate an antibiotic policy for the ICU. This also avoids unnecessary use of broad-spectrum empirical antibiotics and prevents emergence of drug resistant bacterial strains (14). In this study, the highest staphylococci isolation (47.3%) was obtained in cardiovascular surgical ICU which is followed by general surgical ICU (45.1%), burn center (39.8%), coronary ICU (39.4) and internal ICU (33.9%). There was statististically significant difference between surgical ICUs and internal ICUs (p<0.05, Figure 1). The burn units are very susceptible habitats to bacterial colonization (8). Distribution of MRSA strains on units was different. Methicillin-resistance rate was 86.5% (32/37) in burn center. Also it was 84.9% (45/53) in general surgical ICU, 81.5% (22/27) in cardiovascular ICU, 70.5% (31/44) in internal ICU, and 66.7% (14/21) in coronary ICU (Figure 2). Methicillin susceptibility rate with respect to units, however, was obtained highest in internal ICU (64.7%, 11/17). It ranged from 28.6 to 36.4% in other ICUs (Figure 3). ICUs are generally considered epicenters of antibiotic resistance and the principal sources of outbreaks of multi-resistant bacteria. The most important risk factors are obvious, such as excessive consumption of antibiotics exerting selective pressure on bacteria, the frequent use of invasive devices and relative density of a susceptible patient population with severe underlying diseases (14). Vancomycin and teicoplanin have been considered the only available antibiotics uniformly active against multidrug-resistant staphylococci. Therefore, reports of staphylococci with reduced susceptibility to these agents are alarming. In 1997, Hiramatsu et al. described the first clinical S. aureus isolate with intermediate resistance to vancomycin (15,16). Later, similar strains with reduced susceptibility to vancomycin were identified in Europe and the United States (17). The emergence of CoNS strains with reduced susceptibility to glycopeptides has also been described (18, 19). It is reported an increased incidence of CoNS isolates with decreased susceptibility to teicoplanin in hospitals where glycopeptide agents are widely used (20). In this study, none of the MRSA and MSSA as well as coagulase negative and coagulase positive staphyloccocci showed resistance against vancomycin. Penicillin resistance was found to be 100% in MRSA while it was 76% in MSSA. There is significant difference between two groups (p<0.05). Resistance of MRSA and MSSA against teicoplanin was 14.7% and 8.3% respectively, while it was 10.5% and 8.7% for MRCoNS and MSCoNS, respectively. In acquiring resistance against teicoplanin, there was no statistical difference between two groups in terms of methicillin resistance or susceptibility (p<0.05). A similar event was observed for trimethoprim-sulphamethoxazole. In developing resistance against trimethoprim-sulphamethoxazole, there was no statistically significant difference between MRSA (529.9) and MSSA (20.8%), and MSCoNS (42.9%) and MRCoNS (45.1%) (p<0.05, figure 4,5). In terms of acquiring resistance against all antibiotics (gentamicin, erythromycin, clindamycin, norfloxacin, ofloxacin, penicillin), there was significant difference between MRSA and MSSA (p<0.05, Figure 4,5). The isolation rate of staphylococci was found to be high in patients treated at ICUs. Methicillin resistant and susceptible staphylococci cause seriously high infection risks at burn units as well as other ICUs. Antibiotic resistance of MRSA strains was found to be higher than that of MSSA. In ICUs, empirical antibiotic treatments should be avoided and treatment should be carried out using antibiotic susceptibility tests. ICUs should be regularly inspected for MRSA colonization which shows great resistance pattern against antibiotics. Colonization of ICU patients with antimicrobial-resistant pathogens can lead to clinical infection because of breakdown of normal host defenses. ICU patients are particularly susceptible to nosocomial infection because the normal skin and mucosal barriers to infection are commonly compromised by the use of invasive devices (21). We recommend regular screening of ICUs patients to give an early warning of the presence of antimicrobial-resistant pathogens and allow the assessment of barrier and infection control techniques. Such monitoring also can aid the infection control in determining how to focus its efforts in reducing the emergence and spread of antimicrobial resistant pathogens. Data derived from global surveillance studies can provide important information about the changing spectrum and regional variation of antimicrobial resistance patterns. This information can be used to assist in the design of empirical treatment regimens and also to plan control measures for emerging antimicrobial-resistant staphylococci. In conclusion, we suggest that the most important strategies for controlling the problem of multidrug-resistant organisms in any ICU should be directed towards continuously monitoring the presence of these organisms, and the avoidance of excessive or continued use of any single drug over a long period of time. REFERENCES
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}