 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
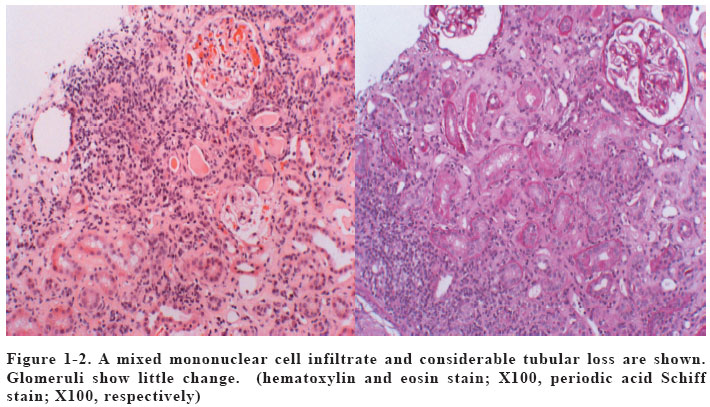
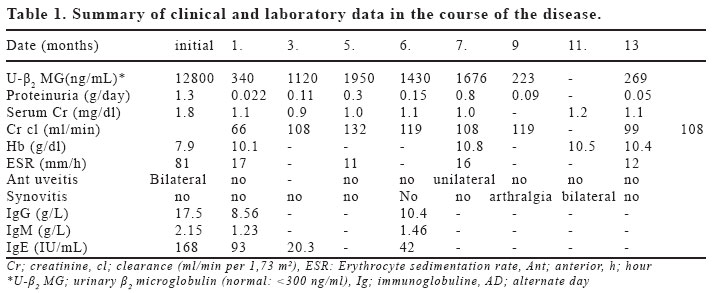
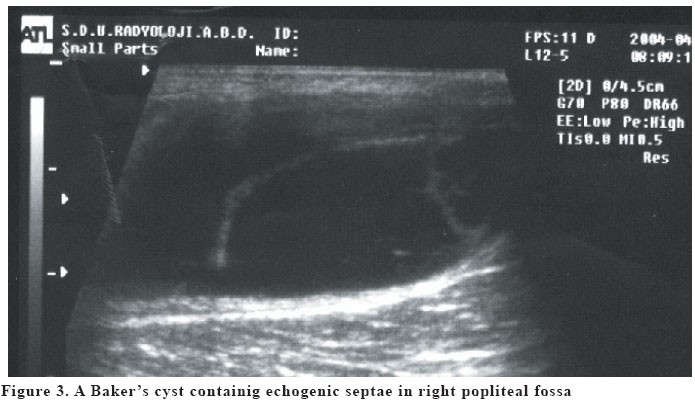
European Journal of General Medicine, Vol. 2, No. 1, 2005, pp. 27-31 TUBULOINTERSTITIAL NEPHRITIS AND UVEITIS SYNDROME WITH SYMMETRICAL SYNOVITIS IN A MALE ADOLESCENT Faruk Öktem1, Şevket Ercan Tunç2, Şeref Olgar1, Yavuz Bardak3, Bahar Kılınçarslan4, Gülten Karpuzoğlu4 Suleyman Demirel University Faculty of Medicine, Departments of Pediatrics1, Internal Medicine2 and Ophtalmology3, Isparta, Turkey. Akdeniz University Faculty of Medicine, Department of Pathology4, Antalya, TurkeyCorrespondence: Dr. Faruk Öktem 239 cad. No:19 Tıbbiyeliler sitesi, Binbirevler Isparta, Turkey Phone: +90 246 2112211, Fax: +90 246 2370240 E-mail: oktemfaruk@hotmail.com Code Number: gm05006 We report a case of tubulointerstitial nephritis and uveitis (TINU syndrome) in a 16-year-old male adolescent. He had weakness, anorexia, weight loss and malaise. He had no ocular symptom at presentation. Impairment of renal function, tubular proteinuria, anemia, increased erythrocyte sedimentation rate, eosinophilia and hypergammaglobulinemia were detected. He had HLA-DR4, HLA-A3 and HLA-B51 positivity. HLA-B27 was negative. The renal biopsy showed interstitial cell infiltrates and tubular atrophy without granulomas in interstitium. Glomeruli showed mild mesangial hypercellularity. Immunofluorescent staining was uniformly negative. After administration of systemic corticosteroids, renal, ocular and constitutional manifestations regressed. Bilateral knee arthritis developed 2 months after stopping the steroid treatment and in which ultrasonography showed a Baker's cyst in right. Oral sulfasalazine was started and local corticosteroid was injected into the cyst. Symmetrical synovitis regressed without taking systemic steroid treatment. TINU syndrome should be considered in the differential diagnosis of patients presenting with non-specific constitutional, visual and renal manifestations. During the follow-up, synovitis may develop rarely. This is the first case report of TINU syndrome with symmetrical synovitis and Baker's cyst. Key words: Tubulointerstitial nephritis, uveitis, synovitis INTRODUCTION The tubulointerstitial nephritis and uveitis (TINU) syndrome was first described in 1975 by Dobrin et al. as a new and distinct entity in two adolescent female patients with acute eosinophilic interstitial nephritis, anterior uveitis, and noncaseating granulomas in both bone marrow and lymph nodes (1). Etiological factors and the pathogenetic mechanisms in TINU syndrome are unclear (2, 3). Some HLA subtypes are reported to be associated with this rare syndrome (4). It commonly presents with non-specific constitutional symptoms such as fever, malaise, weight loss, anorexia and fatigue. The differential diagnosis includes infections, drugs, toxins and multisystem illness (2,3). The median age of onset was 15 years with a 3:1 female-to-male predominance (3). Persistent renal dysfunction, ocular complications and chronic course may appear in some cases (5). Treatment is controversial but patients are usually treated with systemic corticosteroids and immunosuppressive drugs and the renal outcome in children is usually good but uveitis tends to follow a relapsing course (2,3). Here we report another case of TINU in an adolescent male developed symmetrical synovitis and whose renal findings and uveitis improved after treatment with systemic corticosteroids. CASE A 16-year-old male presented with a 2-years history of general malaise, anorexia, fatigue and pallor. He had no history of another disorder and a drug treatment. His complaints had increased gradually in last 2 months and in this period he had lost 6-kg. On admission he had no blurred vision and redness in eyes. Three months prior to admission, he was diagnosed as iron deficiency anemia. In physical examination, pallor and fever (between 37-38.2 oC) were present. He was normotensive. The weight and stature of case were 46.5 kg (10th percentile) and 170 cm (over the 97th percentile). He had no joint symptom, organomegaly and lymphadenopathy. Ophthalmological examination which is done for routine investigation revealed bilateral nongranulomatous anterior uveitis. Urinalysis showed 8-10 leukocytes per high-power field and 1-2 granular casts without erythrocytes, and a sterile culture. Hypercalciuria and aminoaciduria were absent but glucosuria and proteinuria were present. Urinary β2-microglobulin was found high. Laboratory studies showed: leukocytes 8,200 /µl with 12% eosinophils, hemoglobin 7,9 g/dL, hematocrit 28,5 %, the mean cell volume of erythrocyte 87.4 fL (N: 80-94), platelets 631x103/µL, reticulocyte count 2/103, ferritine 63,6 mg/dL, serum iron 23 µg/dL, serum iron binding capacity 144 µg/dL. Laboratory investigation showed a high erythrocyte sedimentation rate (ESR), C-reactive protein 87 mg/L (normal:<6 mg/L), serum creatinine 1.8 mg/dL, creatinine clearance 57 ml/min per 1,73 m2, blood urea nitrogen 39 mg/dL, uric acid 4.3 mg/dL, calcium 9.3 mg/dl, sodium 139 mEq/L, potassium 4.5 mEq/L, chloride 103 mEq/L, total protein 8.1 g/dL, albumin 3.9 g/dL, globulin 4.2 g/dL, total cholesterol 123 mg/dL, trigliceride 66 mg/dL. Table displays serum immunoglobulin levels. Anti-nuclear antibody, anti-neutrophil cytoplasmic antibody, antids-DNA, anti-Sm antibodies, anti-Ro, anti-La, anti-U1RNP, and anti-SCL-70 antibodies, rheumatoid factor, Coombs tests, antiperoxidase and antithyroglobulin antibodies were all negative. Serological tests for hepatitis B, C, human immunodeficiency virus, cytomegalovirus, rubella, herpes simplex and Epstein-Barr virus were negative. Thyroid hormones were normal. Bone marrow examination revealed no granulomatous lesion. Chest X-ray was normal. Abdominal ultrasonography showed evident bilateral enlargement of the kidneys with high echogenicity. A percutaneous renal biopsy was performed on hospital day 8. Portions of 18 glomeruli were seen by light microscopy. Glomeruli showed mild mesangial hypercellularity. An eosinophylic hyalinized material accumulation and mild endotelial cell proliferation was seen on vascular walls. There were focal thickening of the basal membranes and focal narrowing in Bowman's space. There were eosinophils, lymphocytes and plasma cell infiltrates associated with focal tubular atrophy and fibrosis in interstitium. In the areas of cellular infiltration, lymphocytes were seen to be entered into the fragmented tubular walls. T lymphocytes found in cellular infiltration were stained positive for CD4 and CD8. The CD4+ lymphocytes were slightly more than CD8+ ones. Immunofluorescence investigation showed no evidence of immune complex deposition. These findings are in accordance with the diagnosis of tubulointerstitial nephritis (Figure 1, 2). Despite treatment with topical steroids, no regression occurred in uveitis within 5 days. Following renal biopsy, alternate day intravenous pulse methylprednisolone (30 mg/kg/dose, maximum 1 gr/dose) treatment was administered for three times and oral methylprednisolone treatment continued in the dosage of 48 mg/day for four weeks. Then, gradually decreased to 40 mg, 20 mg, 12 mg and 4 mg alternate-day dosages for every month. Urinary β2-microglobulin and serum creatinine decreased to normal. The creatinine clearance was improved to 107 ml/min per 1.73 m2. Corticosteroid dosage was decreased to a dosage of 4 mg in alternate day in 6 months of follow up and in this period unilateral uveitis recurred. And also, urinary β2-microglobulin level increased (Table 1). Therefore, methylprednisolone dosage was increased to 16 mg/ alternate day, proteinuria and uveitis improved in 2 months and corticosteroid treatment was stopped gradually. After 2 months, bilateral knee arthritis developed and ultrasonography showed a Baker's cyst in right (Figure 3). The uric acid levels were normal at the time of the arthritis. Sulfasalazine 1.5 gr. daily begun and local corticosteroid (triamcinalone acetonide) was injected into the cyst. His symmetrical synovitis regressed. Currently, he continues to have sulfasalazine 1.5 g daily. At the last visit, autoimmune profile repeated at the time of active arthritis. Only rheumatoid factor was found 28 IU/ml, (normal range: 0-15 IU/ml) the others were negative. At present, 15 months after our first observation, the patient is free of uveitis and tubular proteinuria without taking oral corticosteroids. DISCUSSION Tubulointerstitial nephritis and uveitis is a rare syndrome, which occurs predominantly in adolescent girls (2). However, there have been an increasing number of reports of male patients in the recent literature (3). The median age of onset is 15 years. It is not associated with any racial or ethnic group (3). Patients with this disorder are characterized by uveitis, nephropathy, biochemical abnormalities and marked constitutional symptoms. The uveitis is typically anterior, bilateral, and nongranulomatous. It often relapses, but long term ocular sequelae are rare (3,6). The most common ocular complaints were eye pain, redness, decreased vision and photophobia. Eye symptoms may precede, be simultaneous with or follow the nephropathy (2). Although usually symptomatic, it can also occasionally be asymptomatic as our case. Anterior uveitis is the diagnostic clue to the syndrome. Nephropathy is characterized by tubular function impairments and an acute decrease in renal function. Tubulointerstitial nephritis is characterized by interstitial edema and infiltration by mononuclear inflammatory cells, including lymphocytes, eosinophils, plasma cells and histiocytes (7). Immunofluorescence microscopic studies have been uniformly negative for tubulointerstitial and glomerular various immunoglobulins or complement deposits, including stains for IgE. Glomeruli are normal or show minimal mesangial prominence, but the vessels are found normal. Acute intertitial nephritis has been associated with a wide variety of drugs, toxins, infectious agents and autoimmune disorders (7,8). Biochemical abnormalities include increased serum creatinine levels, erythrocyte sedimentation rate, immunoglobulins, and anemia. Reason of anemia may occur due to chronic systemic disease. Because MCV of patient was found normal. The pathogenesis of this ocular-renal disorder has remained unclear, but likely involves an autoimmune reaction against constituents common to the renal tubulointerstitium and uveal tract (7,9). TINU syndrome appears to be a systemic disease associated with alterations in T cell-mediated immune mechanisms (10). The T-cell proliferation within the kidney in the acute interstitial nephritis confirms this, as observed in our patient. The elevated immunoglobulin levels detected in our case, as well as those from the literature, also represents an involvement of B lymphocytes. Several studies have also reported that human leukocyte antigen (HLA) specificities of patients with TINU syndrome (3,4,7). The most commonly reported HLA specificities are HLA-A2, HLA-A24 and HLA DR6 (4, 7). Our patient had HLA-DR4, HLA-A3 and HLA-B51 positivity. This result may be the result of ethnic origin of our patient. But, the number of reported cases is insufficient for a statistical analysis to assess the relative risks associated with reported HLA specificities. TINU syndrome must be part of the differential diagnosis of every patient that presents with either idiopathic interstitial nephritis or uveitis. There are no specific diagnostic tests; therefore TINU is a diagnosis of exclusion (2). A number of disorders including infections and collagen tissue diseases can cause both renal disease and uveitis. But the majority of these disorders do not result in anterior uveitis alone, which is the most common ocular manifestation of TINU syndrome (2,3). Kidney biopsy in early stages could show a picture like interstitial nephritis with ocular problems in patients with nephronopthisis. The recovery of renal function and presence of uveitis rule out this diagnosis. Tubulointerstitial nephritis may be caused by drugs, infectious agents, and immunological disorders. There was no history of drug treatment in our case, particularly of non-steroidal anti-inflammatory drugs, which are known to predispose to interstitial nephritis. Our patient presented with non-specific symptoms such as subfebrile fever, general fatigue, weight loss and general malaise. Treatment of this rare syndrome is controversial, and outcome in children compared to adults is excellent. Corticosteroids seem essential in treating these patients (9,10). However, systemic steroid therapy does not seem necessary for all patients, there is some evidence that renal function may improve more rapidly in steroid-treated patients (2,3,8). Our patient had bilateral uveitis, significant tubulointerstitial injury and decreased renal function. Therefore, we used long-term systemic steroid. Two months after improvement of proteinuria and uveitis he had developed bilateral knee arthritis. Ultrasonography showed a Baker's cyst at right side which regressed after intralesional corticosteroid injection and sulfasalazine treatment. In the course of sulfasalazine treatment he had no new joint symptom. In literature, symptoms indicative of rheumatoid arthritis or sacroiliitis have been reported in the follow-up period (11,12). But, to our knowledge, this is the first report of TINU syndrome developing symmetrical synovitis with a Baker's cyst in the follow-up period. This rare and late clinical manifestation of TINU syndrome improved with sulfasalazine and local steroid treatment alone, without systemic corticosteroids. TINU syndrome should be considered in the differential diagnosis of patients presenting with non-specific constitutional, visual and renal manifestations. It is probably an under-diagnosed disorder. The presence of renal dysfunction in patients with uveitis may be of some help, as a warning sign, for the rapid recognition of patients. The TINU syndrome is a readily treatable disease with corticosteroids. In some untreated patients, permanent renal and ocular damage may develop. Considering this case report, anti-rhematic drugs as sulfasalazine may be of additional benefit to TINU patients, particularly in rheumatic manifestation. REFERENCE
Copyright 2005 - Medical Investigations Society The following images related to this document are available:Photo images[gm05006t1.jpg] [gm05006f3.jpg] [gm05006f1-2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}