 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 1, 2005, pp. 32-34 INFANTILE OSTEOPETROSAIS SSOCIATED WITH RICKETS Yaşar Bükte1, Fuat Gürkan2, Mehmet Davutoğlu2, Ayfer Gözü2, Meki Bilici2 Dicle University Medical Faculty, Departments of Radiology1 and
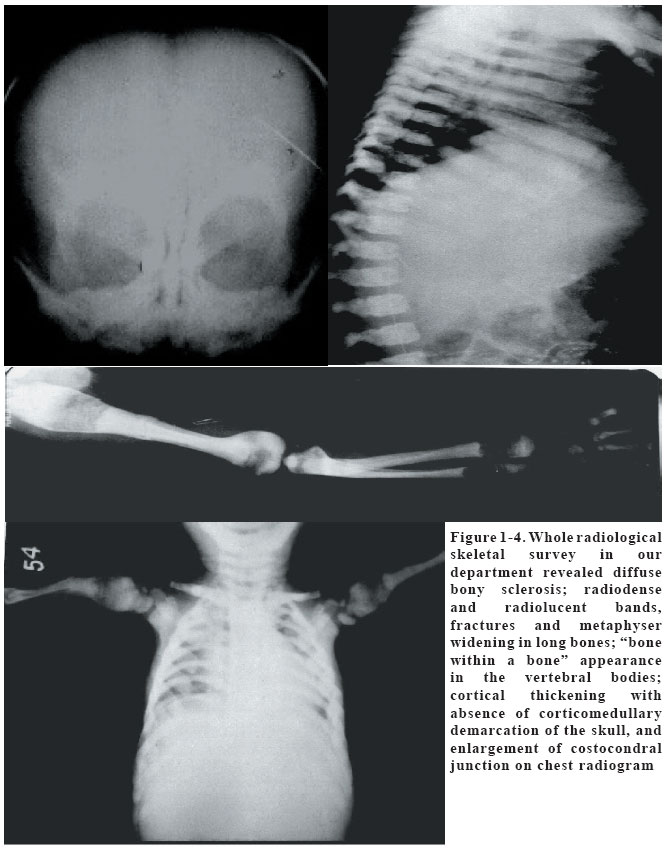
Pediatrics2 Diyarbakır, Turkey Code Number: gm05007 A 3-year-old female child was diagnosed as malignant autosomal recessive form of infantile osteopetrosis by presence of anemia, thrombocytopenia, hepatosplenomegaly, failure to thrive, visual and hearing loss, and the typical radiological images on plain radiograms. The patient had associated clinical and laboratory findings of rickets as a rare presentation. Treatment with calcitriol was initiated with a short-term calcium supplement. Key words: osteopetrosis, infant, rickets INTRODUCTION Infantile osteopetrosis is a rare hereditary bone disease characterised clinically by multiple fractures, abnormally shaped bone, and anaemia. The most serious consequences are seen in the nervous system such as cerebrovascular complications, cranial nerve palsies and optic nerve atrophy. Although the disease is characterised by increased skeletal mass and bone density and a positive balance of body calcium, a paradoxical association with rickets has rarely been reported (1). We herein present such a case with osteopetrorickets with typical clinical and radiological findings. CASE A 3-year-old female child, product of a consanguineous marriage came to examination for symptoms of fever and cough. She had a prior history of hospitalization from pneumonia at another center ten days before her current admission. She neither spoke nor walked upto that time but she was not investigated for these symptoms. The parents informed of their suspicion of the child's blindness as well. At presentation to our department, she was pale; hair was hypopigmented and sparse; there was frontal bossing, malar prominence, depressed nasal bridge, wide open anterior fontanelle, widening of wrists, prominence of the costochondral junction, and pectus excavatus. Abdomen was distended with organomegaly (both liver and spleen were 5 cm below costal margin). She had a fever of 380C and pulmonary auscultation revealed bilateral fine inconstant inspiratory crackles. Weight and height measurements were less than 10th percentile, and her head was macrocephalic (>97th percentile). Fundus examination showed bilateral optic atrophy. Laboratory investigations revealed: hemoglobin 6.9 g/dl, white blood cells 13700/mm3, platelets 127000/mm3, serum calcium 8.8 mg/dl, serum phosphorus 3.4 mg/dl, serum alkaline phosphatase 395 IU/L, serum 25-hydroxyvitamin D level <10 ng/ml (normal range: 10-50) and serum parathyroid hormone level 148 pg/ml (normal range: 8-70). Brainstem auditory-evoked potential was then performed and the results showed bilateral absence of auditory-evoked responses, which strongly suggested bilateral deafness. Whole radiological skeletal survey in our department revealed diffuse bony sclerosis; radiodense and radiolucent bands, fractures and metaphyser widening in long bones; "bone within a bone" appearance in the vertebral bodies; cortical thickening with absence of corticomedullary demarcation of the skull, and enlargement of costocondral junction on chest radiogram (Fig 1-4). There was irregularity and indistinct fraying at the tip of the ulna. The patient was diagosed as infantile osteopetrosis associated with rickets and initiated calcitriol of 1 µg/day and oral calcium supplement of 375 mg/day in our department. The dose of calcitriol was planned to be gradually increased to 2,4 and 8 µg/day every 15 days over a period of 3 months, but the patient was not brought to routine controls and she fell from follow up afterwards. DISCUSSION Osteopetrosis is a rare condition characterized by accumulation of excessive bone mass due to defective bone resorption. Four clinically forms are recognized-the infantile malignant autosomal recessive form, the intermediate autosomal recessive form, autosomal recessive form with renal tubular acidosis and the adult benign autosomal dominant form (2). Patients with autosomal recessive osteopetrosis is diagnosed in early infancy and has a fatal prognosis (3). In our case, the positive findings leading to the diagnosis of malignant autosomal recessive form of infantile osteopetrosis were the presence of anemia, thrombocytopenia, hepatosplenomegaly, failure to thrive, visual and hearing loss, and the typically described radiological images on plain radiograms. The clinical and radiological findings are characteristic, but diagnosis may sometimes be overlooked as in our patient. At the referring hospital, plain radiography of the chest was priorly assessed as rachitic pneumopathy and pneumonic infiltration; and anemia and thrombocytopenia was considered as findings of megaloblastic anemia, since the patient had remarkable feeding problems. To establish a diagnosis, neurological findings in association with positive radiological signs on whole skeletal survey should be investigated in malnourished children who have nonspecific signs of anemia and hepatosplenomegaly. The most serious consequences of osteopetrosis are seen in the nervous system. Cranial nerves, blood vessels and the spinal cord are compressed by either gradual occlusion or lack of growth of the skull foramina (4,5) Osteopetrosis is a rare hereditary bone disease with intense positive balance of body calcium. Association with rickets is not expected to be so common, because the calcium balance is just opposite in rickets (6,7). We think that rickets is not a common and variable feature of osteopetrosis, but the reason for the association of two disorders is that both are seen in populations where consanguinity is more common and there are also many nutritional problems leading to low calcium intake and poor intestinal absorption. As a paradoxical complication of infantile osteopetrosis, rickets may also result from the inability of the osteoclasts to maintain a normal calcium-phosphorus balance in the extracellular fluid (8). Despite a markedly positive total body calcium, the serum calcium and phosphorus may not be sufficient to mineralize the newly formed osteoid leading to rickets. In osteopetrosis the patients are often advised to reduce calcium intake; but in osteopetrorickets, patients need calcium supplementation because of limited calcium intake and poor intestinal absorption (1,8). For this reason we have also initiated treatment with calcitriol and calcium supplementation in our patient. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}