 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 1, 2005, pp. 35-38 RHEUMATOID ARTHRITIS AND PULMONARY CARCINOID TUMOR Mehmet Sayarlıoğlu1, Mustafa İzmirli2, Kürşat Uzun3, Süleyman Alıcı1, Reha Erkoç1 Yüzüncü Yıl University Medical Faculty,Departments of
Internal Medicine1 and Radiation Oncology2, Van, Turkey,
Selçuk
University Medical Faculty, Department of Pulmonary Diseases3,Konya,
Turkey
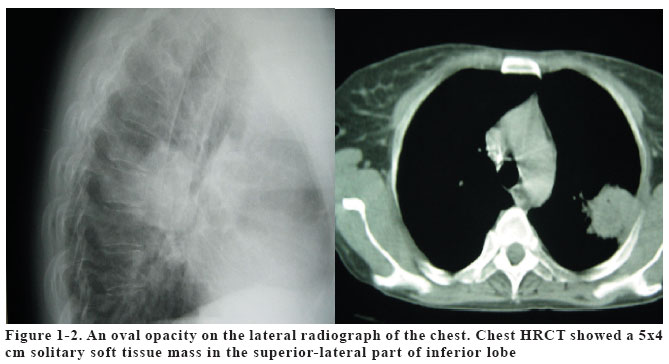
Code Number: gm05008 A 40-year old woman was admitted with a history of elbow, wrist, knee pain and prolonged morning stiffness. Rheumatoid arthritis (RA) diagnosed before five years, had been treated with non-steroidal anti-inflammatory agents and low dose corticosteroid. On hospital admission, routine chest x-ray showed a 4x4 cm solitary mass in the right pulmonary. A diagnostic thoracotomy was performed. The histological examination showed a typical carcinoid tumor. This is the third carcinoid tumor case reported to be associated with RA. Key words: Rheumatoid arthritis, carcinoid tumor INTRODUCTION Rheumatoid arthritis (RA) is a chronic, autoimmune disease of unknown etiology, characterized by symmetrical polyarthritis resulting in damage to cartilage and bone. It is estimated to have a worldwide prevalence of 1%, with a 2- to 3-fold excess in females and a peak in prevalence between the ages of 45 and 54 years (1). Several studies have described an increased risk of malignancy in subjects diagnosed with RA (2). Carcinoid tumors of the lung, such as of the intestinal tract, are derived from neuroendocrine Kulchitsky cells located within the bronchial or intestinal mucosa (3). Bronchial carcinoid tumors account for approximately 2% of all lung tumors (3,4). Two cases of carcinoid tumor associated with RA were reported before (5,6). In this case report, we described a patient in whom RA concurred with pulmonary carcinoid tumor. CASE A 40-year old woman was admitted in March 2003 with a history of elbow, wrist, knee pain and prolonged morning stiffness. RA, had been diagnosed in 1998, had been treated with non-steroidal anti-inflammatory agents and low dose prednisolone, in doses of 5-10 mg/day. The patient was noncompliant i.e. had not take her drugs properly and come to her follow-up visits regularly and she also had not taken any disease modifying anti-rheumatic drug. On admission body temperature was 36.6 ºC, and pulse was 80/min, her blood pressure was 118/75 mmHg. Musculoskletal examination showed mild swelling and tender of the metacarpophalengeal and proximal interphalengeal joints of the hands, which also showed mild ulnar deviation. The elbows, wrist and knee were mildly tenderness. There was no subcutaneous nodule. Rest of the physical examination was normal. Laboratory results were as follows: erythrocyte sedimentation rate 70 mm/h, serum CRP 39 mg/dl, white blood cell count 9.000 /mm3, platelets 320.000 /mm3, haemoglobin 12.5 g/dl, haemotocrit 38 %, BUN 13 mg/dl, creatinine 0.8 g/dl. Rheumatoid factor was 430 IU/ml. ANA, c-ANCA, and p-ANCA were negative. Urinalysis was normal. Tuberculin skin test was negative. Joint x-ray showed the marked erosions of the carpal, metacarpophalengeal and proximal interphalengeal joints. On hospital admission routine chest x-ray showed a 4x4 cm solitary mass in the right lung (Figure 1) which was confirmed by high resolution computerized tomography (HRCT) scan. Chest HRCT showed a 5x4 cm solitary soft tissue mass in the superior-lateral part of inferior lobe (Figure 2). No mediastinal lymph node was noted. Bronchoscopy and bronchoalveolar lavage analysis were normal. A CT-guided transthoracic needle aspiration was performed and cytologic examination of the obtained specimen could not revealed the exact nature, but findings did not suggest any infection, rheumatoid nodule or malignancy. The nature of the nodule in this case cannot be determined from the clinical, radiographic findings and microscopic examination. Diagnostic thoracotomy was performed. Macroscopic examination showed a 4 cm brownish mass located in the superior-lateral part of the inferior lobe. The mass was well limited. A right inferior lobectomy was performed thus the tumor was totally resected. Microscopically, the diagnosis was carcinoid tumor of the lung. After the operation, evaluation of urinary 5-hydroxyindoleacetic acid showed a normal value. Upper and lower abdominal computerized tomography did not reveal any carcinoid tumor originating from gastrointestinal tract. The patient was followed without any treatment for carcinoid tumor. DISCUSSION Pulmonary carcinoids are classically located as single nodules close to hilus, and rarely they present peripherally and exceptionally multifocal (7). Symptoms of carcinoid tumors can be highly variable and are often present for many years before diagnosis (8). Approximately one-third of the reported patients were asymptomatic, and their tumors were discovered on routine chest radiographs (4,9). In symptomatic patients, the most common clinical findings are those associated with bronchial obstruction, such as persistent cough, hempotysis, and recurrent or obstructive pneumonitis. Wheezing, chest pain, and dyspnea also may be noted (4,8,9). In our case a single mass in right lung was revealed by routine chest x-ray of the patient without any symptom. The carcinoid syndrome, which may include flushing, diarrhea, abdominal cramping, wheezing, and carcinoid heart disease, is rare (2.6%) (8). The symptoms result from the synergistic interaction between 5 hydroxytryptamine metabolites, kinins, and prostaglandins released by the tumour into the general circulation. There is no clinical finding related to carcinoid syndrome in our case. Among patients with RA, there was an increased risk for hematopoietic, lung and prostate cancers and a reduced risk for colorectal cancer (10,11). Several mechanisms have been suggested for the association between RA and the increased risk of hematopoietic malignancies including tissue alteration, chronic lymphocyte stimulation and action of immunosuppressive therapy, though risks have been observed in RA patients who have not received immunosuppressive therapy (12). The substantial decrease in risk for colon and rectum cancer in patients with RA or osteoarthritis is believed to be a consequence of treatment with non-steroidal anti-inflammatory drugs (13). In most cases, typical carcinoid tumors characteristically grow slowly and tend to metastasize infrequently (5-10%) (8). Therefore, we could not to establish which is started first; RA or CT. First probability is the development of RA before carcinoid tumor. It was known that RA increases the likelihood of pulmonary tumors (2). But in the literature there is only one case report (5) regarding the association of pulmonary carcinoid tumor and RA. In this case carcinoid tumor was diagnosed 3 years later after the development of RA. The percentage of carcinoid tumors among lung cancers is very low (3,4). It is very difficult to suggest a relation between RA and carcinoid tumor with only two cases. Other possibility is the development of carcinoid tumor after RA. As neuroendocrine tumors, carcinoids are capable of producing a variety of biologically active pepdides and hormones, including serotonin, adrenocorticotropin hormone (ACTH), antidiuretic hormone (ADH), melanocyte-stimulating hormone, and others. Carcinoid tumors of the bronchus may be source of ectopic-hormone secretion and such patients may present with Cushing's syndrome. Carcinoid tumors of the bronchus may also secrete ADH and, infrequently, growth hormone releasing hormone (14). Animal studies support that neuroendocrine factors may effect the development of chronic inflammatory diseases. Defects in the hypotalamic-pituitary-adrenal axis in Lewis rats predispose them to experimental chronic inflammatory joint disease, as well as a wide spectrum of autoimmune or hyperimmune responses, depending on the nature of the inducing agent (15,16). Multiple non-ACTH factors are involved in regulating adrenocortical functions. These include neurotransmitters, neural and nonneural neuropeptides, cytokines, growth factors, and vascular endothelial molecules (17). Additionally several lines of evidence suggest that hormones play a role in the pathogenesis of RA (18,19). Although there is no symptom related to carcinoid syndrome was present in our case, some biologically active peptides or hormones produced by the tumor may be triggered the development of RA. In the literature there are two RA (5,6) and two ankylosing spondylitis (AS) (20,21) cases were reported in association with carcinoid tumors (Table 1). One of the AS case's symptoms was started with carcinoid syndrome symptoms and it was suggested that AS development may be triggered by the carcinoid tumor (21). In other AS case (20) and RA cases (5,6) carcinoid tumor was diagnosed after the rheumatologic diagnoses. One of the RA patient had pulmonary carcinoid tumor and the other had ileocecal carcinoid tumor. These associations are either incidental or there may be a relation between RA and carcinoid tumor. When RA and carcinoid tumor incidences considered, the likelihood of being coincidence seems more logical. Existence of new case reports or series in the literature including coexistence of these two diseases may elucidate the exact nature of this relation. REFERENCES
Copyright 2005 - Medical Investigations Society The following images related to this document are available:Photo images[gm05008f1-2.jpg] |
| |||||||||

{kind=link}