 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 2, 2005, pp. 43-46 PROFILE OF BEHCET’S DISEASE AT VAN AND VICINITY Ömer Çalka1, Necmettin Akdeniz1, Ahmet Metin1, Hayriye Sayarlıoğlu2 Yüzüncü Yıl University, Faculty of Medicine, Departments of Dermatology1 and Internal Medicine2, Van,Turkey Correspondence: Ömer ÇALKA, MD YYU Tıp
Fakültesi Araştırma
Hastanesi Dermatoloji AD 65200 Van, TURKEY Code Number: gm05010 Aim: Behcet’s disease is a chronic, progressive
disease with an unknown etiology and involves many organs and systems. Although
the disease can be encountered at different regions on earth, prevalence and
clinical findings of the disease may demonstrate differences due to local and
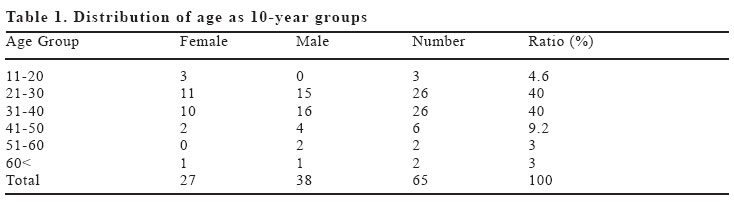
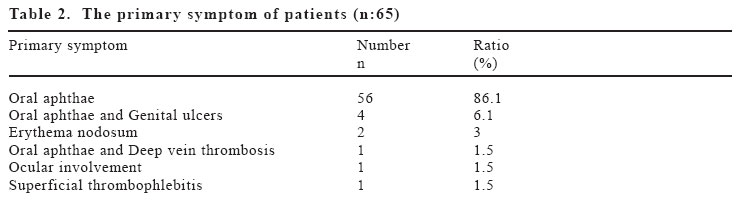
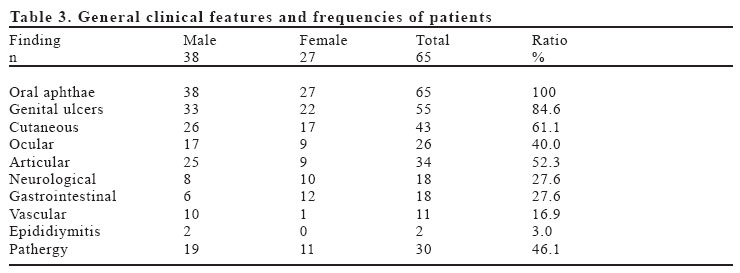
geographical specifications. Keywords: Behcet’s disease, clinical features, Van. INTRODUCTION Behcet’s disease (BD) is a chronic, progressive disease with an unknown etiology, and involves many organs and systems (1). At 1937 the table of symptoms defined as “repeating oral and genital ulcerations and iridocyclitis accompanied with hypopyon”that was described by the Turkish dermatologist Hulusi Behcet at 1937 was first called “The 3-Symptom Complex of Behcet’s”and after then named as “BD”(1-4). Symptoms of the disease were recognized previously by many scientists, but were commonly evaluated as findings related with tuberculosis, syphilis, rheumatism or staphylococcal allergic condition (2). Although the disease can be encountered at different regions on earth, prevalence and clinical findings of the disease may demonstrate differences due to local and geographical specifications. The present study was scheduled to display the mentioned variations. However, presently there was no local information concerning the disease at the vicinity. MATERIALS AND METHODS In the present study, data obtained from 65 cases who were diagnosed to as BD according to the criteria reported by the International Behcet’s Disease Working Group (5) among 29063 consecutive patients referred to our outpatient clinic in the past four years. Patients were assessed according to age, sex, age of onset, site of arrival, family history, any hospitalization due to BD, pathergy test and clinical findings of the disease. RESULTS Within the period that covers the study the number of cases diagnosed with BD was 65 (0.2%), whereas the number of common policlinics was 29063. Thirty eight of the cases were men (58.4%) and 27 cases were women (41.5%). The ratio of men/women was 1.4. The age of cases varied between 16-72 years and the mean age was 32.8 (mean for men:33.4, mean for women: 31.3). Nearly 80% of the cases were between 21-40 years old when the distribution of age was considered as 10-year groups (Table 1). The duration of the disease changed from zero to 32 years and the mean was found 6.4 years. The age of the patients differed between 15-58 years when diagnosed to have BD while the mean age was determined as 26.7 (mean for men: 28.6, mean for women: 24.9). When the settlements of the patients was investigated, 27 patients came from Van City Center (41.5%), 24 from various districts or villages affiliated with Van (36.9%), 4 from Hakkari (Province) (6.1%), 3 from Bitlis (Province) (4.6%), 2 from Ağrı (Province) (3.0%) and 5 from other districts (7.6%). Thirty-five patients (53.8%) were hospitalized once or more due to BD and received treatment. The primary symptom was oral aphthae in 56 patients (86.1%) while oral aphthae and genital ulcer were present in 4 patients (6.1%), erythema nodosum (EN) in 2 patients (3%) and oral aphthae and deep vein thrombosis (DVT) in 1 patient (1.5%), ocular involvement in 1 patient (1.5%) and superficial thrombophlebitis (STP) in 1 patient (1.5%) (Table 2). Oral aphthae was observed in all of the 65 patients (100%), while genital ulcer was determined in 55 patients (84.6%), cutaneous findings in 43 patients (61.1%), ocular involvement in 26 patients (40%), articular symptoms in 34 patients (52.3%), neurological involvement and gastrointestinal (GIS) involvement each in 18 persons (27.6%), vascular involvement in 11 patients (16.9%), epididymitis in 2 patients (3%) and positive pathergy in 30 patients (46.1%) (Table 3). The oral aphthous lesions were minor in 32 patients (49.2%), major and minor in 22 patients (33.8%), major in 7 patients (10.7%) and herpetiform type in 4 patients (6.1%). There were two or more synchronized aphthous lesions in 55 (84.6%) patients and, mostly were located at the lips (89.2%), tongue (86.1%) and the cheek mucosa (85.1%). Genital ulceration was detected in 55 patients (84.6%), 33 of these cases were men (60%) and 22 were women (40%). At the same time, 39 patients (70.9%) demonstrated single lesion while two or more lesions were present in 16 patients (29.1%) synchronized. The lesions were mostly located at the scrotum (87.8%), then at the corpus in men (21.2%); and at the labium major (77.2%) and at the labium minor in women (31.8%). Additionally, an inguinal location was determined in two male patients. Ocular involvement was observed in 26 (40%) patients, 17 (65.3%) of them were men and 9 (34.6%) were women. The majority of the patients displayed a lesion as anterior and/or posterior uveitis, secondary cataract or retinal vasculitis. In 3 patients partial, and in 1 patient complete blindness occurred. Thirty-four (52.3%) patients displayed a joint involvement. Twenty-five (73.5%) of these patients were men while 9 (26.4%) were women. The majority of the patients had arthralgia while 4 patients suffered from arthritis and 1 from sacro-ileitis. Gastrointestinal symptoms, such as abdominal pain and diarrhea, were present in 12 females (66.6%) and 6 males (33.3%), making a total number of 18 cases. Among 11 patients with vascular retention, 10 (6.9%) patients were males and 1 (9%) patient was a female. All most commonly located at the extremities, superficial thrombophlebitis (STP) developed in 7 and STP and DVT in 2 patients and only DVT in 3 patients. DVT accompanied with oral aphthous lesions was noticed in 1, and STP in 1 patient as a primary finding of the BD. Twenty-six (60%) of the patients out of 43 (61.1%) who displayed dermal findings were males while 17 (39.5%) were females. In this group, for 34 patients (79%) papulopustular lesions, for 4 patients (9.3%) papulopustular lesions and EN, and for 5 patients (11.6%) only EN were detected. Papulopustular lesions were located at the legs and at the upper region of the trunk, predominantly on the back while EN was observed on the legs of the patient. Neurological findings -mainly headache- were present in 18 patients (27.6%). Ten of the patients (55.5%) were females while 8 (44.4%) were males. Epididymitis was found only in 2 (3%) male patients. The pathergy test was assessed as positive in 30 patients (46.1%). Nineteen (63.3%) of the patients were males and 11 (36.6%) were females. DISCUSSION BD is a multisystem disorder with a pathological priority of vasculitis. The etiology of the disease is not known clearly, but it is assumed as an autoimmune reaction in individuals who were stimulated by viral, bacterial or other antigens and who have a genetic predisposition (1-3). BD is a disorder that can be seen worldwide, but the diversity of its frequency reminds us the possible role of environmental factors. The disease is more frequent in the Mediterranean vicinity, where Turkey is included. Mid-East and Japan and has a prevalence about 1-10/10.000; BD is less frequent in Northern Europe, USA and Australia and the prevalence is approximately 1/300.000 (3,6). In our country the ratio of prevalence in adults was 8/10.000 (7) in villages nearby to Istanbul by Demirhindi et al, 37/10.000 (8) at Çamaş/Ordu by Tüzün et al and 4.09/10.000 (9) at Doğankent/Adana by Acar et al for entire age groups. Nevertheless, this study is not a reliable prevalence study, but a ratio of 22/10.000 among patients who referred to our outpatient clinic may give an idea. Ural et al and Aytekin et al found different ratios of prevalence at near provinces by using the same method, respectively, 31/10.000 (10) for Erzurum and 8.2/10.000 (11) for Diyarbakır. The preliminary age of onset of BD begins at 20-40 years of age and is more frequent in men (1,6). The preliminary age of onset of BD in our study was between 15-18. The mean age was 26.7 while 80% of the cases were included in the 21-41 years old group. The F/M ratio was 1.4. Although there is not any absolute evidence related with an inherited passage of the disease, familial cases were reported (12). Four of our patients (6.1%) revealed familial anamnesis. Findings related with oral aphthous and genital ulcers in our patients are compatible with the findings in the literature (3,4,6,10,11). Other clinical findings display a general parallelism to literature data. However, among our patients, ocular involvement was 40% while this ratio was reported previouslyas 50-58% (3,6), and the ratio of cutaneous lesions was 66.7% while this ratio was previously reported as 70-80% (3,13) and the ratio of neurological retention was 27.6% while this ratio was reported previously as 1-20% (3,13). A portion of this difference may be dependent to the diversity of researchers who were evaluating findings at the time the study was performed and another portion can be dependent to regional and local environmental factors. We thought that, this first description of data about BD in Van and vicinity might be helpful to researchers. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}
{kind=link}
{kind=link}