 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 2, 2005, pp. 47-55 THE OUTCOME OF MAJOR HEPATECTOMIES FOLLOWING DIFFERENT DURATIONS OF PORTAL VEIN LIGATION IN RATS Ertan Bülbüloğlu1, Mustafa Şahin2, Bülent Kantarçeken3, Harun Çıralık4,Ali Çetinkaya3, Fatma İnanç5, Fikret Ezberci1 1Sütçü İmam University, Faculty of Medicine, Department of General Surgery Kahramanmaraş, 2Vakif Gureba Training Hospital, Department of Surgery, İstanbul, Sütçü İmam University, Faculty of Medicine, Departments of Gastroenterology3, Pathology4 and Biochemistry5, Kahramanmaraş, Turkey Correspondence: Ass.
Prof. Dr. Ertan Bülbüloğlu Kahramanmaraş Sütçü İmam
Universitesi, Tıp
Fakültesi, Genel Cerrahi Bölümü 46050 Kahramanmaraş ,Turkey Code Number: gm05011 Aim: Atrophy/Hypertrophy complex constitution (AHC) by
portal vein ligation (PVL) before major hepatectomies (Hx) has got beneficial
effects on the functional capacity of the remnant liver tissue by increasing
its volume. We aimed to evaluate whether longer duration of PVL has any additive
benefit on regenaration speed, weight, biochemical, histological examination
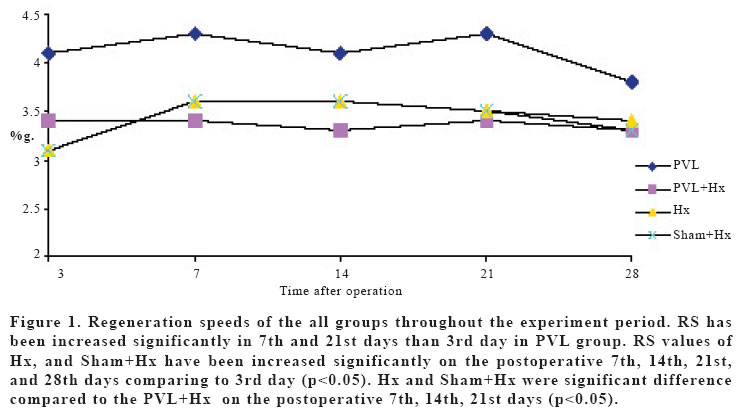
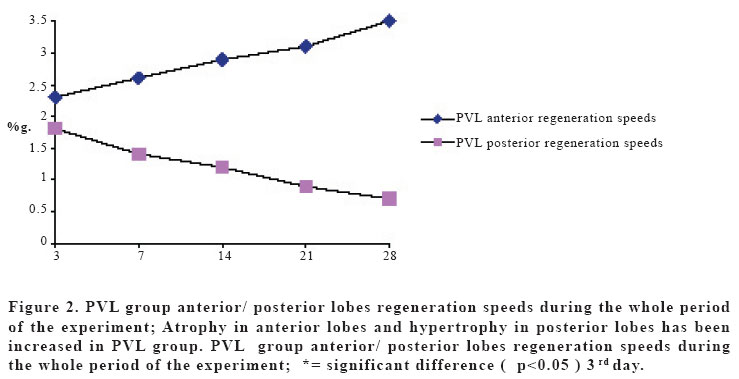
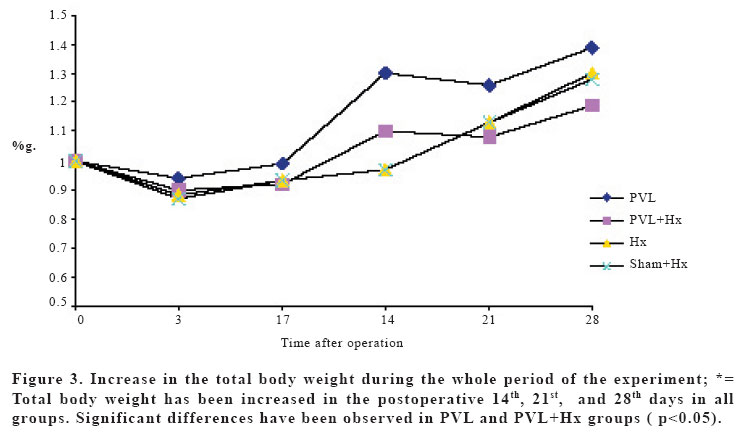
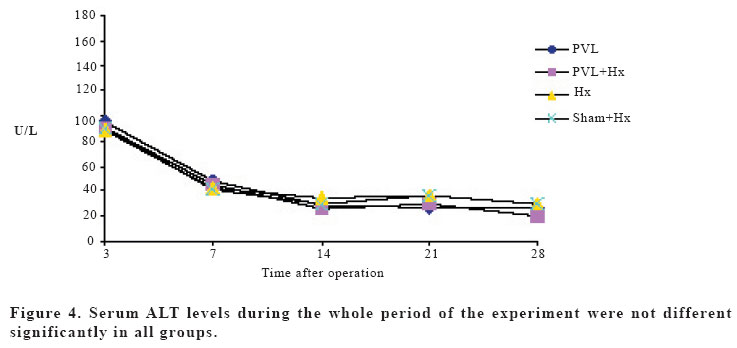
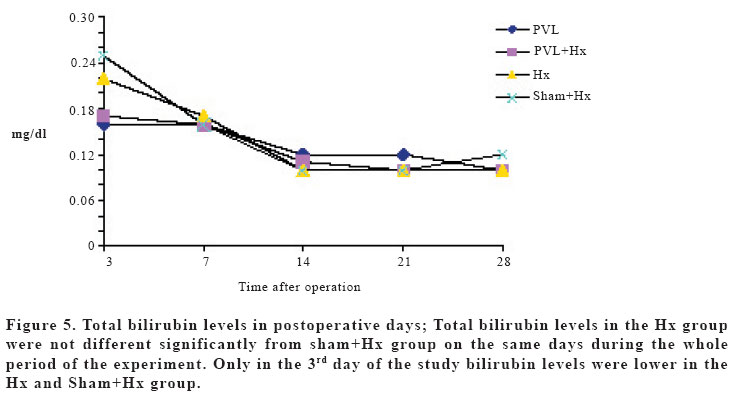
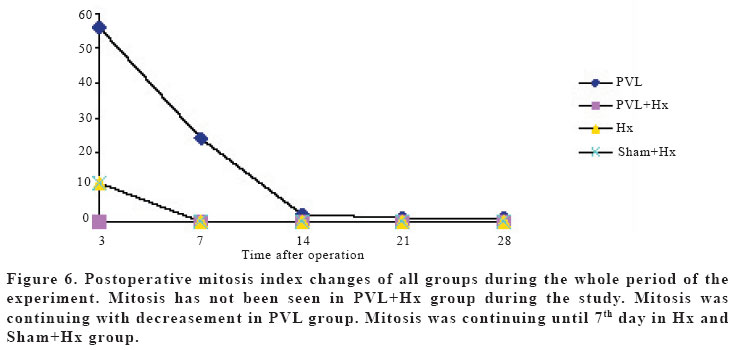
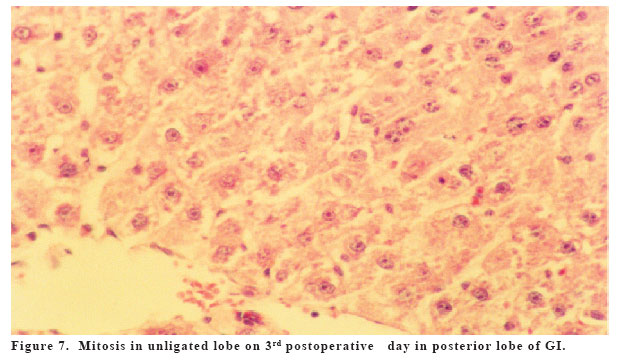
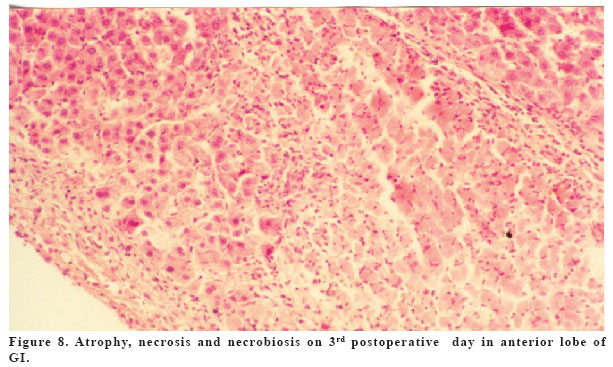
and mortality, before major hepatectomies in rats. Key words: Portal vein ligation, Atrophy, Hypertrophy, Hepatectomy, Liver, Rat. INTRODUCTION Major hepatectomies has been done not only in malign pathologies of the liver, but also in benign liver pathologies. After major hepatectomies ( Hx ) due to benign or malign causes, if the remaining tissue is not enough hepatic failure risk leads to increased risk of morbidity and mortality in postoperative period (1-9). It is known that portal blood carries the materials having trophic effects that cause hypertrophy and hyperplasia (10,11). In animal and human experiments, after the ligation of portal vein, atrophy has been observed in the same side of ligation and hypertrophy in the opposite side (Atrophy/Hypertrophy complex (AHC) (12-18). It has been shown that hx is safer by constituting AHC (12,13). It has been shown that in PVL constituted rats for 28 days the atrophy in ligated lobes and hypertrophy in non-ligated lobes last significantly. Longer term PVL constitution in benign pathologies is not a severe problem as in malign pathologies, such as growth of the tumor. To our knowledge there’s no report about major Hx after long term PVL in rats in the litherature. This paper presents the results of major Hx in AHC constituted rats after a longer duration of PVL. MATERIAL AND METHOD This study was performed in experimental examination laboratory of Inonu University. 120 Wistar Albino rats (weight between 180-200 gr, heterogenous) were used for the study. Rats were fed with laboratory feed and normal water. Two hours after the operation the rats had been fed with the laboratory feed, normal water and 30% Dextrose solution for three days. All operations were performed under steril conditions between 8 and 11 a.m for the standardization of diurnal changes. Before the operations the rats had been kept as starved for 12 hours. Anesthesia was induced with ketamine hydrochlorur (50 mg/kg, im, Ketalar,® Parke-Davis). Laparotomy was performed with upper abdominal incision. 120 rats were divided into four experimental groups, each containing 30 rats (PVL, PVL+Hx, Hx, Sham+Hx). PVL; laparotomy and PVL, PVL+Hx; 70% Hx and relaparotomy after 21 days from PVL, Hx; Laparotomy and 70% Hx, Sham+Hx; 70% Hx and Relaparotomy after 21 days from Sham ligation. PVL was performed as the ligation of the left portal vein leading to the anterior lobe. Hx was performed via the technique that was described by Higgins and Anderson (19). In the Sham ligation group, left branch of the portal vein was dissected, but the procedure was finished without ligation. For preventing any postoperative hypovolemia, 5 ml NaCl was given to the peritoneal cavity and abdomen was closed by 4/0 silk double layer continue. Rats died in first two days were excluded from study. The groups were formed from the remaining rats. Each group were divided into five subgroups according to the examination times after procedures ( a, b, c, d, e ). Number of rats diminished in all groups due to deaths, and the smallest number of rats were left in subgroup e. The G-I ( PVL ) had 6 rats in each subgroup, G-II (PVL+Hx) had 6 rats in subgroups a,b,c,d and 5 rats in subgroup e. G-III (Hx) had 5 rats in each subgroup. G-IV (Sham+Hx ) had 5 rats in subgroups a,b,c,d and 4 rats in subgroup e. All rats were kept starved for 12 hours and weighted after procedures. Rats were sacrified with cervical dislocation and 3 ml blood was taken by cardiac punture for biochemical tests. Anterior and posterior lobes of the liver were excised separately and weighted wetly and then put into 10% formalin solution for histological examination. Postoperative following parameters 1. Regenaration speed (RS); the percentage of the ratio of the wet liver weight of sacrified rat (LW) to the total body weight (BW) was accepted as “RS”value (RS=LW/BW.100). With this formula the RS values of all rats were calculated. Then, the arithmetic mean value of each subgroup was determined. Also, standart deviations (SD) of the values were calculated for each subgroups. 2. Weight: All rats were weighed on 3rd, 7th , 14th , 21st and 28th days before procedures. Mean weight and standart deviation (SD) of each subgroup was determined. 3. Biochemical evaluation; Serum alkaline phosphatase and total bilirubin were measured in blood samples (Syncron Cilnical System CX4 (® Beckman). 4. Histological examination; Liver tissue specimens were routinely fixed and stained with Hematoxylene - Eosine. Mitosis index was accepted as the mean value of mitosis number in 10 different areas with 40 microscopic scale. The arithmetic mean value of mitosis index of each subgroup was accepted as the mitosis index of the subgroup. 5. Mortality: Died rats during the study were evaluated. Statistical analysis All data were expressed as mean+SD. The statistical differences in each group were determined by the analysis of variance, using Wilcoxon Matched-Pairs Singned Ranks test, differences between the groups were determined by using Mann-Whitney U test. Mortality rates were evaluated by Chi-square test. RESULTS Mean Operation Time The mean operation duration were; 10, 15, 13, and 14 minutes in PVL, PVL+Hx, Hx, and Sham+Hx respectively. Regeneration speed (RS) Regeneration speeds of the groups throughout the experiment period were shown in the Figure 1. PVL, and PVL+Hx groups did not show significant increasement in RS values compared to 3rd day. RS values of Hx, and Sham+Hx had been increased significantly on the postoperative 7th, 14th, and 21st days compared to 3rd day (p<0.05). The RS of anterior and posterior lobes of the liver of PVL group were shown on Figure 2. PVL group anterior/ posterior lobes regeneration speeds throughout the whole period of the experiment were significant difference compared to 3rd day (p<0.05). Weight changes in rats The weights of the rats were decreased 6%, 10%, 12%, 13% in groups PVL, PVL+Hx, Hx, and Sham+Hx, respectively on the third postoperative day. Decreasement of weight in each group on the third day was statistically significant (P<0.05 in each group). After the third day of operations an increasement in the weights was observed and on the seventh postoperative day the weights of the rats were reached preoperative values. The weights of the rats were increased as 39%, 19%, 30%, 28% in groups PVL, PVL+Hx, Hx, Sham+Hx, respectively on the 28th postoperative day (Figure 3). Biochemical results The serum alkaline phosphatase and total bilirubin levels of the study groups were shown in the Figures 4 and 5. Serum alkaline phosphatase levels were increased in all groups postoperatively, and started to decrease in the postoperative 7th day and returned to normal values. The increasement in serum alkaline phosphatase levels did not show significant difference compared with the whole groups. Bilirubin levels were lower in PVL and PVL+Hx groups than Hx and Sham+Hx groups in 3rd day of the study. Mitosis index Mitosis was observed on the 3rd day in the Hx and Sham+ Hx group and on the 14th ,day in PVL group. There was not any mitosis in PVL+Hx during the study.Mitosis was observed in the Hx and Sham+Hx on 3rd day but there was not in PVL+Hx (Table 6). Histopatological examination Hyperplasia, hypertrophia and mitosis were observed in posterior lobe in PVL, but mitosis was not observed in anterior lobe. Atrophy, increase of connective tissue and bile duct proliferation had been observed until 28th day in anterior lobe. Necrosis in anterior lobe had been continued for seven days postoperatively (Figure 1,2). Mortality Mortality rate was significant lower in PVL and PVL+Hx groups than Hx and Sham+Hx groups. Rats were died due to liver failure at first two days. DISCUSSION Enough functional remnant tissue is essential for decreasing postoperative morbidity and mortality risk in major hepatectomies (1,4-7). Liver has extremely good regeneration ability and this ability is controlled with hepatotrophic factors and inhibitor agents (14,20-26). It has been known that vena portae carries hepatotrophic factors (Insulin, glucagon etc.) (15,27-32). Atrophy in ligated lobe and hypertrophy in opposite lobe have been observed in human and animals and this was called Atrophy/Hypertrophy complex (AHC) (14). At least two hypothesis have been suggested about the controlling of cell proliferation triggering in liver resection. First, self-inhibition mechanism; With the decrease in inhibitory factors by resection, the remnant tissue proliferes quickly (22-24). Second; Cell to cell contact inhibition gets lost and proliferation occurs due to activation of regeneration stimulators in suboptimal remnant liver tissue (15,22). Schweizer et.al (14) had constituted AHC model in rats. They had shown that AHC occurred with PVL and/or PVL with ligation of one of ductus hepaticus together, but not with ligation of a ductus hepaticus alone. In this study AHC have been constituted with only PVL. The regenaration speed and duration of the liver is directly associated with the volume of the resected liver tissue (20). It has been shown that the liver reaches in normal dimension in one week after 70% hepatectomies (15). In Alison’s study (15), atrophy had been observed in ligated lobe in 15 hours and liver had reached the 80% of the total weight after 3 days from ligation with hyperplasia in opposite lobe. With a similar study it has been shown that non-ligated lobe had reached the 63%, 75%, 89% of the total liver weight on the 3rd, 6th, 18th days, respectively (15). On the contrary of the resection groups GIII and GIV, regeneration speed has not been changed in GII in our study. It is thought that regeneration speed does not change after Hx when 70% Hx is performed in rats constituted AHC after long term (21 days) PVL. Because the tissue that will be resected is relatively very small in atrophic side after PVL. For starting the regenerative response of the liver, at least 10-20% of the total liver tissue must be resected (20). Regenerative response has not been occured because of the relatively small resection of the liver tissue in GII, in our study. Regenerative response might have been observed if PVL duration had been shorter as in Chjiiwa’s study (32). The weight of the rats reached to preoperative values on 7th day and increased 38% on postoperative 28th day. Results were similar with AHC by PVL in Schweizer’s study (14), but there was less decreasement in the weight of the rats on 3rd day in our study. This may be originated from nutrition with 30% dextrose solution (5cc/day). It has been shown that hypertonic dextrose solutions decrease mortality by increasing regeneration in rats performed major hepatectomy. Dextrose effects regeneration by increasing the secretion of hepatotrophic insulin (29). Similarly in Gaub and Iverson’s feeding rats model study, survive of the rats was increased to 80% with postoperative glucose solution (32). Increasement in wet weight of the liver is not only associated with hyperplasia. It has been shown that the quick increasement in weight in unligated lobes of rats soon after first 24 hours then PVL is more associated with increased portal pressure and hepatic congestion than hyperplasia and this condition has not been observed only in hepatectomies. It has been shown that portal pressure was increased on first days of PVL and then peaks in 4th day and returned normal after ten days (28). Alkaline phosphatase levels in the studies in which major Hx was performed after having constituted AHC were decreased to normal range on 2-7 days, as in our study (27). Similar histopathological examinations on 3rd day of our study, Rous and Larimore had shown necrotic lesions in ligated lobe in 1920 (16). Rozga et al. (10) had shown the complete resorbtion of necrosis by monocytes on 4th day in rabbits. Also, Rozga et al. (11) had shown contracted arterial branches in tissue specimens 72 hours after PVL. Daniel and Prichard had shown that this condition was associated with reflex vasocontruction (31). Adkison et al. (33) had reported that free oxygen radicals originated from ischemic reperfusion damage due to vasoconstriction would cause necrosis. Unexplained connective tissue increasement and bilier duct proliferation is seen with atrophy in the ligated lobe. After ligation, edema and inflammation follow tissue damage in early period. This causes expansion in interstitiel compartment. Then, increasement in connecting tissue is observed. Granulation tissue occures in necrotic tissue at first and then connective tissue increases (14). Atrophy, destruction, involution and decrease in weight have lasted until postoperative 3rd day in ligated lobe. Hypertrophy in opposite lobe has lasted until postoperative third day, too. In our study, mitosis has not been seen in PVL+Hx group during the study. Mitosis was continuing with decreasement in PVL group. Mitosis was continuing until 7th day in Hx and Sham+Hx group. In this study mortality has not been seen in rats that were constituted AHC. Mortality rates were significant lower in PVL and PVL+Hx groups than Hx and Sham+Hx groups. The mortality in Hx was associated with the volume of the resection 30. We could suppose that a decrease in mortality may occur if liver resection is done later in the rats that have been performed portal vein ligation, in order that the less tissue have to be resected. In this study the relatively lesser liver tissue that was resected in the rats that were constituted AHC by long term PVL (Associated directly with the duration of the PVL) led more enough remnant liver tissue to maintain normal function of the liver with lesser mortality rates. As a result, PVL should be performed longer time before major hepatectomies for decreasing the postoperative complications and mortality with enough functional capacity of liver in benign liver pathologies. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}