 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 2, 2005, pp. 76-79 HYPOCALCEMIA INDUCED RHABDOMYOLYSIS AND ACUTE RENAL FAILURE AFTER THYROIDECTOMY: A CASE REPORT Ömer Toprak, Atilla Üzüm, Rıfkı Ersoy, Mustafa Cirit Department of Nephrology, Ataturk Research and Training Hospital, Izmir, Turkey Correspondence: Ömer Toprak, MD 163.Sok.No:4 35170
Kemalpasa-Izmir TURKEY Department of Nephrology, Ataturk Research
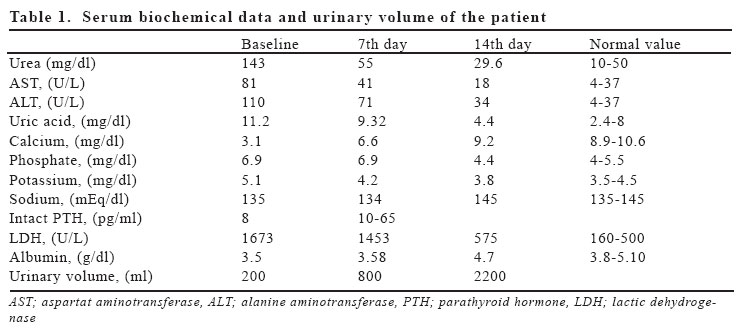
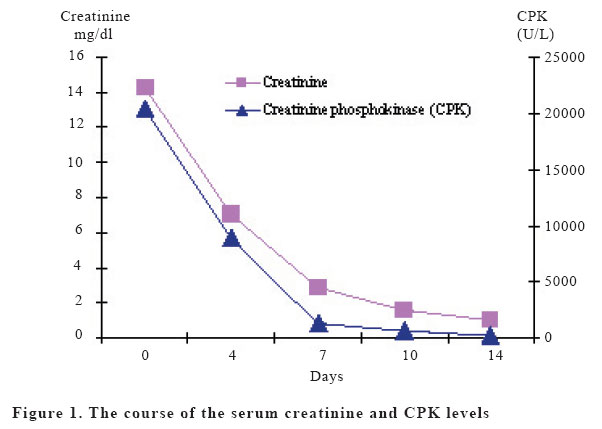
and Training Hospital, Izmir, Turkey Code Number: gm05015 Rhabdomyolysis is a potentially life-threatening syndrome resulting from the breakdown of skeletal muscle fibers with leakage of muscle contents into the circulation. We report a case of a 24-year-old woman with hypocalcemia which occured after a thyroidectomy operation. This hypocalcemia was severe enough to cause convulsion, rhabdomyolysis and acute renal failure. The reason of severe hypocalcemia in our case may be multifactorial; hypoparathyroidism, rhabdomyolysis and acute renal failure. The development of hypocalcemia, convulsion attacks, rhabdomyolysis and acute renal failure occurring in the patient after iatrogenic hypoparathyroidism has rendered the case interesting due to the rarity of such developments. Key words: Acute renal failure, convulsions, hypocalcemia, iatrogenic hypoparathyroidism, rhabdomyolysis. INTRODUCTION Iatrogenic hypoparathyroidism is a complication which can be observed after thyroidectomy operations, at an average ratio of 5 % (1). If no supportive treatment is given, hypoparathyroidism could lead to a severe hypocalcemia causing convulsions (2). The spectrum of causes of rhabdomyolysis includes a wide array of diseases and disorders. The most frequent causes are muscle compression, alcohol abuse, hereditary metabolic derangements, drugs and infections. Rhabdomyolysis may develop in patients with convulsions due to muscle damage. Rhabdomyolysis is an important risk factor for the development of acute renal failure (ARF) (3). Rhabdomyolysis forms around 10 % of all the ARF cases (4,5). In this report, a case has been presented and literature have been searched, due to its rarity, where the developed hypocalcemia, after a thyroid operation, was severe enough to cause convulsions, rhabdomyolysis and ARF. CASE A 24-year-old woman was admitted to our hospital because of high fever and reduced urinary output. She had a history of bilateral subtotal thyroidectomy operation due to toxic nodular goitre three weeks ago and recurrant convulsion attacks for five days after the operation. Examination revealed bilateral pre-tibial oedema, Chvostek and Trousseau positivity, and an operational scar on the neck. Blood pressure of 150/90 mmHg, axillary temperature of 380C and respiratory rate of 20/minute were observed. Other examination findings were normal. Laboratory investigations were as follows; leucocyte: 10400/mm³ (86% neutrophils) and haemoglobin: 10.9 g/dl, urine color was dark, density was 1015, urinary dipstick was positive for blood, 1-2 pigmented casts and 5-6 leucocytes were present but no red blood cell was seen in urinary sediment. Other abnormal biochemical results have been shown in table 1. Ciprofloxacin sensitive E.Coli grew on the urine culture. Hemoculture was negative. Her arterial blood gases revealed metabolic acidosis (pH: 7.29, HCO3: 17.5). QT prolongation (0.48 sec) was detected in the electrocardiogram. The renal ultrasound was normal. Taking into account all of these findings the patient’s diagnosis was acute renal failure occured after rhabdomyolysis which was caused by the convulsions due to iatrogenic hypoparathyroidism resulting from the thyroid operation. Lower urinary tract infection was also observed in the patient. The patient underwent haemodialysis for two times. Calcium, mannitol, bicarbonate infussion, thyroid hormone replacement, 1,25 dihidroxycholecalciferol and ciprofloxacin treatments were given to the patient. The patient, whose urine output progressively increased and laboratory values become normal (Table 1), had no new convulsion attacks and no haemodialysis was required. The course of the serum creatinine and creatinine phosphokinase (CPK) levels were shown in Figure 1. The patient, whose general condition improved, was discharged from hospital after maintenance therapy. DISCUSSION The development of hypoparathyroidism after thyroid operations is one of the most frequent reasons of postoperative hypocalcemia. It was shown in studies carried out on patients after thyroidectomy, that in about 0.3-3.5% of cases, severe hypocalcemia developed due to hypoparathyroidism and permanent hypocalcemia was observed in only 0.5-1% of cases (1,3). We think that the main reason of the hypocalcemia in our case is iatrogenic hypoparathyroidism. As well as hypoparathyroidism, rhabdomyolysis and ARF may also have had a role in the development of severe hypocalcemia in our patient. Hypocalcemia is the most commonly encountered electrolyte abnormality in rhabdomyolysis. It occurs very early in the course of the disease. It is usually self-limited and rarely requires therapy. Together with the possibility of hypocalcemia occurring as a result of calcium accumulation in the damaged muscle tissues during the oliguria stage accompanying rhabdomyolysis cases. Sepsis is also an independent cause of hypocalcaemia and rhabdomyolysis. However, because of negative hemoculture and mild leucocytosis we thougt that our patient had only a lower urinary system infection, but not sepsis. The incidence of hypocalcemia in the reasons of convulsion is 5% (2-4). In convulsion and status epilepticus conditions, rhabdomyolysis may develop as a result of increased muscular activity. In our patient, convulsions occurred due to hypocalcemia and rhabdomyolysis developed as a result of this. Rhabdomyolysis can be defined by the result of clinical and laboratory findings caused by the inclusion of the cell elements from the disintegrating striated muscle into the systemic circulation (5). Most of the cases occur as a result of extensive exercise, trauma, drugs or excessive alcohol use. Other reasons of rhabdomyolysis are; infections, metabolic illnesses, congenital metabolic myopathies, toxins and ischaemia (3). The severity of the illness can vary from the asymptomatic increase of muscle enzyme or severe enzyme increase and electrolyte inbalance to life threatening conditions such as ARF (5). Early hypocalcemia and late hypercalcemia along with hyperphosphatemia have been demonstrated consistently in patients with rhabdomyolysis. The hypocalcemia of the oliguric phase may be secondary to decreased synthesis of 1,25(OH)2D; severe hyperphosphatemia may also have a major role (6). Hypocalcemia is attributed to a variety of causes including: Deposition of calcium in necrotic muscles after binding with phosphate in the circulation. Late hypercalcemia has been reported to occur in rhabdomyolysis induced ARF. The role of parathyroid hormone and 1,25 dihydroxycholecalciferol in calcium homeostasis of rhabdomyolysis had been discussed by different studies (6-8). The calcium is released from damaged muscle and other tissues due to inappropriately high levels of PTH and 1,25-(OH)2-D3 during the recovery period. Hyperphosphatemia, like in our case, seen in rhabdomyolysis due to phosphate leakage from damaged muscle cells results in a decrease in 1,25-(OH)2-D3. The hyperphosphatemia inhibits renal synthesis of 1,25- (OH)2-D3. The elevated phosphates and other organic acids contribute to increased anion gap of rhabdomyolysis (6). The most serious late complication is acute renal failure, which occurs in approximately 15 percent of patients with rahbdomyolysis (4). It has been observed that severe ARF requiring dialysis develops in only 3 % of rhabdomyolysis cases (3,4). Treatment of ARF due to rhabdomyolysis included hydration, alkalinization of urine, diuretics, electrolyte correction, dialysis and supportive therapy. We, therefore treated our patient along these lines. Prompt action must be taken to prevent the complications in a patient with rhabdomyolysis, most importantly aggressive intravenous volume replacement. Effective therapy aims for a urine output of 200-300 ml/hour. If the urine output is sufficient, bicarbonate may be given to maintain an alkaline urine state. This helps to prevent the dissociation of myoglobin into toxic compounds. In an acid urine, myoglobin is toxic and uric acid can crystallize. There are also some concerns about the use of sodium bicarbonate, because it may worsen hypocalcemia or precipitate calcium phosphate deposition on various tissues. Diuretic medications such as mannitol or furosemide may aid in flushing the pigment out of the kidneys. We gived to our patient at a dose of 20 g mannitol twice in a day to maintain urine output. There was no response to the first two boluses, so we didn’t give more. Hemodialysis may be a therapeutic modality. Despite treatment, patients with rhabdomyolysis often develop oliguric acute tubular necrosis. In our patient, despite the theraphy ARF, acidosis and oligo-anuria had developed and thus the patient required haemodialysis. The oliguric period of ARF due to rhabdomyolysis is 7 to 10 days (3). This period in our patient continued for 8 days. The serum parameters of the patient, who responded dramatically to the treatment in the second week, reached totally normal levels, except for a moderate creatinine phosphokinase elevation. As a conclusion, the development of hypocalcemia, convulsion attacks, rhabdomyolysis and acute renal failure occurring in the patient after iatrogenic hypoparathyroidism has rendered the case interesting due to the rarity of such developments. Therefore, patients undergoing thyroidectomy operations should be closely examined in respect to these complications. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}
{kind=link}