 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 2, 2005, pp. 80-82 REPORT OF A GIRL WITH INFANTILE HEMANGIOENDOTHELIOMA Köksal Yuca1, Mustafa Kösem2, Sevil Arı Yuca3, Hayal Oral2, Ali Bay4 Yüzüncü Yıl University Faculty of Medicine, Departments of Otorhinolaryngology1, Pathology2 and Pediatric Heamathology4, Özalp Training Hospital, Clinic of Pediatric Diseases3, Van, Turkey Correspondence: Köksal Yuca, MD, Yüzüncü Yıl
University, Faculty of Medicine, Department of Otorhinolaryngology,
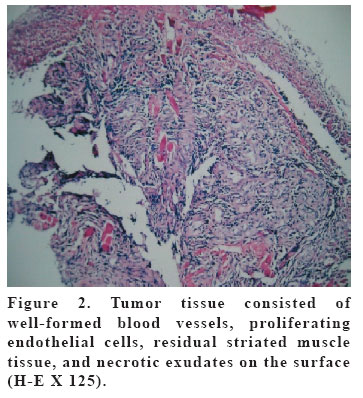
65200, Van-Turkey Code Number: gm05016 Infantile Hemangioendothelioma (IHE) is a rare vascular tumor with predominant involvement of soft tissues of extremities. The occurrence in the head and neck region is extremly rare. We report a four-month-old female with IHE in her lower lip. The clinical and histologic photographs depict the findings. The diagnosis and treatment of IHE are discussed. Key words: Hemangioendothelioma, vascular tumor, infants. INTRODUCTION Infantile hemangioendothelioma(IHE) is a severe disease with a high mortality. It is characterized by multiple hemangiomas affecting the skin and visceral organs (1). Hemangioendothelioma is a rare vascular tumor of endothelial cell origin show an intermediate malignant potential between simple hemangioma and angiosarcoma. The tumor is characterized by neoplastic proliferation of epitheloid or histiocytic endothelial cells. It may involve bone or soft tissues of extremities and can behave like a benign or malignant tumor. The occurrence in the head and neck region is a rare and believed to be a neoplasm of borderline malignancy. In the literature, there are several case reports on the involvement of the head and neck region (2-5). For primary treatment recommendation there is general agreement in the literature as surgical excision of the tumor (2-4, 6). We reported a case of a 4-month old infant with IHE resulted in soft tissue destruction of lover lip and histologic findings were described. CASE A 4-month –old girl with a lower lip mass since birth which began to grow two months ago was admitted to our clinic. Clinical examination showed an ulcerated lesion of 5x2 cm in size in her lower lip, starting from the right mouth commissura, extenting through the midline and vermilion and including a part of the gingiva (Figure 1). No palpable lymphadenopathy was observed in the neck. Outer ear, nose, and throat examination, general physical examination, and routine laboratory investigations showed no abnormalitiy. A punch biopsy was performed under local anesthesia. Histologic examination revealed IHE; the tumor consisted of plump endothelial cells, stromal cells, and residual striated muscle tissue. The surface epithelium was ulcerated. Mitotic figures were scant (Figure 2). Surgical resection was recommended but refused by the patient’s family. The child did not return for any further treatment. DISCUSSION Hemangioendotheliomas are rare vascular tumors show an intermediate malignant potential between simple hemangioma and angiosarcoma (2). The tumor is characterized by neoplastic proliferation of epithelioid or histiocytic endothelial cells. Predominant locations are soft tissues of extremities, the liver and lungs; involment of the head and neck region is a rare (2). The biologic behavior of the tumor appears to be dependent on its location. Mortality from epitheloid hemangioendothelioma in the soft tissues was 13%. As of January 2000 a total of 17 cases with involvement of the head and neck region have been described in the literature; only six case reports with intraoral hemangioendothelioma in the pediatric population have been published(2). Our case had an ulcerated lesion of 5x2 cm in size in her lower lip, starting from the right mouth commissura, extenting through the midline and vermilion and including a part of the gingiva. Outer ear, nose, and throat examination, general physical examination, and routine laboratory investigations showed no abnormalitiy. Hemangioendothelioma is a confusing term. It has been used over the years for vascular tumors composed of endothelial cells, which may involve bone or soft tissues (3, 5, 7). In 1908 Mallory introduced the term hemangioendothelioma (3, 7). Since then, various other synonyms have been adopted including, infantile hemangioendothelioma. Types 1 and 2, celluler angioma of infancy, benign hemangioendothelioma, non malignat hemangioendothelioma, angioendothelioma, lymphangiosarcoma, hemangiosarcoma, angiosarcoma, angioblastoma and intravascular endothelioma (2, 3, 7). Bones of the limbs are most commonly involved. We are aware however, of case reports on the involvement of the head and neck region, as well (3, 5, 7, 8). Our case with a lower lip mass since birth that began to grow at the age of two months was clearly unusal. A definitive diagnosis can be made by means of a biopsy only. Histopathologically hemangioendothelioma is composed of short strands or solid nests of rounded to slightly spindled endothelial cells, which form small inconspicuous lumina, containing erythrocytes. In most cases this tumor shows only mild nuclear pleomorphism and virtually no necrosis or mitotic activity (3). Treatment of hemangioendothelioma usually consist of wide radical surgical excision (2-4,6,8,) with postoperative radiotherapy(3,7), especially in high- grade lesions. Radiation therapy has been used alone when surgery was not feasible (7). Chemotherapy currently has no significant role in the treatment. Orchard et al reported successful treatment with α-interferon in two infants with hemangioendotheliomas, one in the head and neck region (7). In our case; surgical resection was recommended but refused by the patient’s family. In summary due to the confusing nosology with unpredictable biologic behavior and high mortality rate IHE requires close follow-up and urgent surgical treatment of the patient. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}
{kind=link}