 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 2, 2005, pp. 86-88 MAGNETIC RESONANCE IMAGING OF PRIMARY INTRADURAL-EXTRAMEDULLARY THORACOLUMBAR HYDATID CYST Beşir Erdoğmus, Burhan Yazıcı, Betul Ayça Özdere Abant İzzet Baysal University, Düzce Medical Faculty, Department of Radiology, Düzce, Turkey Correspondence: Dr. Besir Erdogmus Abant İzzet
Baysal University, Düzce Medical School, Department of Radiology,
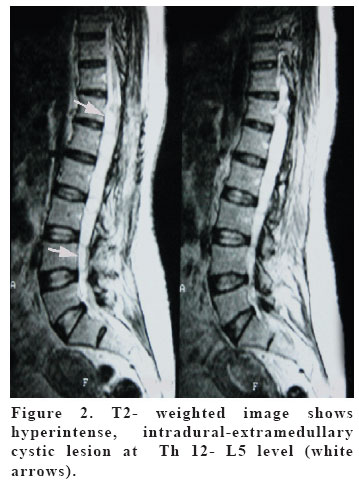
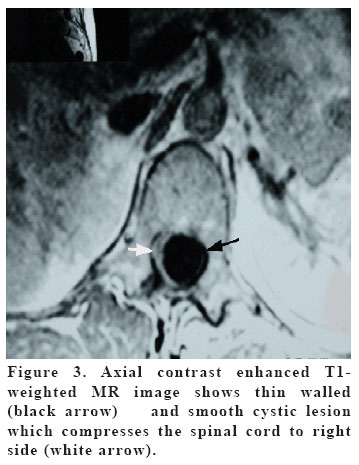
81620 Duzce-Turkey Code Number: gm05018 Hydatid disease (HD) is a parasitic infection. The most affected organs are the liver and the lungs. Spinal HD is rare and constitutes less than 1 % of all HD. Intradural-extramedullary thoracolumbar hydatid cyst is extremely rare. In this report, we aimed to present the magnetic resonance imaging findings of a rare case of primary isolated intradural-extramedullary HD. Key words: Hydatid cyst, magnetic resonance imaging, thoracolumbar, spinal cord INTRODUCTION Hydatid disease is a parasitic disease caused by the larval stage of Ecinnococcus Graulosa (1). Primarily liver and lungs are affected in 78% of all cases but muscles, peritoneum, bone, spleen, pancreas, heart, kidneys and brain are affected only in 22% of cases (2). Spinal HD constitute less than 1% of all HD cases (3). In this report, we aimed to present the magnetic resonance imaging (MRI) findings of a rare case of primary isolated intradural-extramedullary HD with the review of literature. CASE A 43-years old female patient with the symptoms of lumbalgia and numbness in lower extremities for two years was admitted to our hospital. In her physical examination, there was weakness in lower extremities. Lumbar disc herniation was considered as a primary diagnosis, and MRI was carried out. There was a multiseptated intradural-extramedullary cystic lesion which showed hypointensity on T1 WI (Figure 1) and hyperintensity on T2 WI taken from T12 through L5 (Figure 2). After IV gadolinium injection, the lesion did not show contrast enhancement (Figure 3). No pathological sign was detected in the vertebral corpuses, intervertebral disk spaces and paraspinal muscles. We performed abdominal ultrasonography and PA chest radiography in order to find the possible origin of the disease. But both of the examinations were normal. In the serological tests, positive signs of hydatid disease were detected. In respect of these findings, the diagnosis of primary isolated hydatid disease was thought. Our diagnosis was confirmed with the post-operative histopathological examination. DISCUSSION Hydatid disease is known to be endemic in Middle Eastern, Mediterranean, and Australian regions (4,5). Spinal hydatid cyst constitute less than 1 % of all hydatid cyst cases. The distribution of the disease in the spinal area is as: 10% in cervical area, 50% in thoracal area, 20% in lumbar area, and 20% in sacral area (3,6). Spinal hydatid cysts are categorized into 5 groups: 1- intramedullary HC, 2- intradural- extramedullary HC, 3- extradural- intraspinal HC, 4- vertebral HC, and 5- paravertebral HC. The first three groups are extremely rare and they are reported as sporadic cases. In spinal hydatid cysts, pedicles, lamina and spinal canal are invased later on. As there was no foci in the other organs, our case was accepted as primary isolated intradural- extramedullary spinal hydatid cyst and this is extremely rare. In MRI, hydatid cysts are seen as spherical lesions with well defined margins and fine walls (5,6). The fluid content of HC is isointense with CSF on T1 and T2 WI, but the cyst wall is seen as rim shaped which has low signal intensity on T1 WI and T2 WI on MRI. After iv contrast injection, the rim generally does not enhance, and calcification of the wall of the cyst is rare (3). Enhanced ring-shaped wall can be seen if the cyst is infected (1). In our case, no contrast enhancement or calcification was present. In the differential diagnosis of HC, cystic metastasis, abcesses, spondylitis and sacrococcygeal chordoma should be considered. Osteoporosis, sclerosis and intervertebral disk degeneration are seen in tuberculosis, but are not observed in HD (3,7). Chordoma shows a lytic, destructive, mixed solid and cystic lesions. An associated anterior or lateral soft tissue mass is often present (8). Metastasis shows pedicle destruction, multifocal lytic vertebral body lesions, pathologic compression fracture and paraspinous soft tissue mass (9). As a conclusion, primary spinal HD’s are rare (10). Among these, isolated intradural- extramedullary thoracolumbar hydatid cyst cases are extremely rare. In the pre-operative period, MRI is a useful imaging modality in diagnosis of spinal HD and can act a crucial role in the management of treatment. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}
{kind=link}
{kind=link}