 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
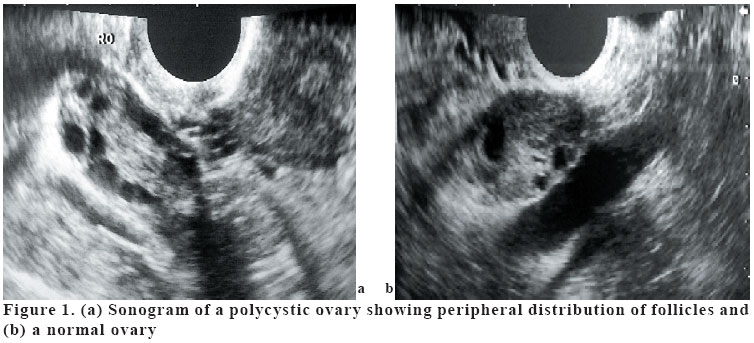
European Journal of General Medicine, Vol. 2, No. 3, 2005, pp. 91-95 EVALUATION OF CEREBRAL BLOOD FLOW VOLUME USING COLOR DUPLEX SONOGRAPHY IN PATIENTS WITH POLYCYSTIC OVARY SYNDROME* Murat Acar1, Serhan Cevrioğlu2, Aylin Yücel1, Bumin Değirmenci1 Ramazan Albayrak1 Alpay Haktanır1 Afyon Kocatepe University, Faculty of Medicine, Departments of Radiology1and Obstetric and Gynecology2, Afyon, Turkey *This paper was presented as scientific poster at European Congress of Radiology 2004 Code Number: gm05020 Aim: Polycystic ovary syndrome (PCOS), one of the commonest endocrinopathies in the human, is known to be associated with risk factors for cerebrovascular disease. The aim of this study was to determine whether there was a change in cerebral blood flow volume in PCOS. Keywords: Polycystic ovary syndrome, Color duplex sonography, cerebral blood flow volume INTRODUCTION Polycystic ovary syndrome (PCOS) is a common reproductive endocrine disorder that is characterized by hyperandrogenism and chronic anovulation, affecting about 5% of premenopausal women (1,2). This syndrome is an important condition associated with risk factors for stroke and coronary artery diseases, including hypertension, insulin resistance, high serum triglyceride levels, and low HDL cholesterol levels (3-6). Although PCOS is associated with risk factors for cerebrovascular disease, the available evidence does not demonstrate increased stroke mortality, and it has been suggested that some protective mechanisms must be operating for these women (7,8). There are many studies which showed hemodynamic changes in the pelvic vessels and aorta in patients with PCOS (1,7,9,10). However, to the best of our knowledge, there have been only three studies concerned with carotid artery hemodynamic changes using color duplex ultrasound in PCOS patients: All three studies were performed by Lakhani et al (7,11,12), which reported lower pulsatility index in the internal carotid arteries (ICA), decreased compliance and increased stiffness of the common carotid arteries (CCA) and ICA, and paradoxical constrictor response to hypercapnia in the ICA in women with PCOS. The principal objective of cerebrovascular Doppler sonography is the analysis and characterization of cerebral hemodynamics under physiologic and pathologic circumstances. In the literature, we could not found any study related to the cerebral blood flow volume in patients with PCOS. In this study, we compare the cerebral blood flow volume in a group of women with PCOS and a matched aged control group of healthy women. MATERIALS AND METHODS Thirty women with PCOS (mean age 24±6 years) and 20 healthy women (mean age 25±5 years) as control group were enrolled. The body mass indexes (BMI) were similar in both groups, 24±4 kg/m² in patients with PCOS and 24±3 kg/m² in control group. The characteristics of the patient and control groups were outlined in Table 1. The cases under 16 or above 35 years of age and whose BMI over 27 were excluded. The cases with PCOS were randomly selected among patients who were admitted to obstetrics and gynecology outpatient clinic with hirsutismus, infertility or menstrual cycle disturbance (oligo-/amenorrhea) whereas the control group was consisted of voluntary hospital staff. Informed consent was obtained before the examination. Ethical approval for the study was granted by the local ethical committee of university. A clinical diagnosis of PCOS was made in the presence of delayed menstrual cycles history (cycle length> 35 days), hirsutismus, and hormonal determinations including raised serum concentration of luteinizing hormone (LH/FSH ratio >2) and/or elevated total serum testesterone (>2.0 nmol/L). Furthermore diagnosis of PCOS was confirmed by the presence of bilateral polycystic ovaries on transvaginal ultrasound; either the presence of 12 or more follicles measuring 2-9 mm in diameter, especially located at the subcortical area of the ovary or increased ovarian volume (>10 cm3) regarded as diagnostic ultrasonographic findings (Fig. 1). Other endocrinopathies that may cause menstrual irregularities or hyperandrogenism such as hyperprolactinemia, thyroid dysfunction, congenital adrenal hyperplasia and androgen secreting ovarian tumors are excluded in PCOS group. The control group included healthy women who had normal ovaries on ultrasound examination, and no evidence of hyperandrogenism (hirsutism or acne). All women in control group had regular menstrual cycles, and none had sought treatment for menstrual disturbances or infertility. Women who had cardiovascular disease and who were smoking or taking oral contraception or other hormonal medications for the last two months were excluded. Examination was performed during the early follicular phase (the first five days) of the menstrual cycle in oligomenorrhoeic and control women; there was no special timing for amenorrhoeic women. Doppler sonography examinations were performed in the morning following at least 8 hours sleep and after having breakfast free of caffeine-containing beverages. All examinations took place in a dimly lighted room with a comfortable temperature (22-240C) after an adaptation period for at least 15 minutes rest in supine position. The ICA and vertebral arteries (VA) of both sides were explored with a 7.5-Mhz linear array transducer of a Toshiba Nemio 20 system. The patient's head was turned slightly to the opposite side each time. Flow volume measurements were generally taken in the C4-C5 intertransverse segment of the VA and 1.5-2 cm distal to the carotid bifurcation on the ICA. Duplex measurement of angle-corrected flow velocities was done with the sample volume expanded over the entire vessel diameter. Visual control of the maximal luminal width and acoustic control of an optimum time frequency Doppler signal made certain that the sample volume passed through the center of the vessel. We aimed to keep the angle of insonation as low as possible, in most cases about 60°. The angle-corrected time averaged flow velocity (TAV) was determined as the integral of the mean flow velocities of all moving particles passing the sample volume over three to five complete cardiac cycles. In this way, the pulsatile parabolic flow is mathematically transformed into a continuous plug flow. The intravascular flow volume (FV) was calculated as the product of TAV and the cross sectional area (A) of the circular vessel using the formula FV=TAV×A=TAV×[(d/2)²×π]. The cross-sectional areas of the ICA and VA were determined as the distance between in the internal layers of the parallel walls. In addition a pulsed Doppler spectral curve was obtained and peak systolic velocity, resistivity index (RI), pulsatility index (PI) were also evaluated. We detected ICA and VA flow volume. The cerebral blood flow (CBF) volume was calculated as the sum of flow volumes in the ICA and VA of both sides. All measurements were documented by black-and-white video printer. The complete examination took about 15 minutes for each case. Data were analyzed statistically by the Student's t test. Correlation between age and flow velocity of ICA and VA were assessed with Pearson correlation coefficients. All parametric results were expressed as mean ± SD for each group. Local statistical significance was assumed as p<0.05 for all parameters. RESULTS The mean ICA velocity, RI, PI and mean VA RI, PI in patients with PCOS and control group were not statistically different (p>0.05). However mean VA velocity in patients with PCOS was lower than control group (46±8 versus 54±14 cm/s, p=0.018). CBF volumes in patients with PCOS and control group were not statistically different. Furthermore the sum of bilateral ICA and VA flow volumes were not significantly different between two groups, as well. Mean±SD values for CBF volumes, sum of ICA and VA flow volumes, mean RI, PI and velocities are shown in Table 1. Correlation between age of patients and flow volume of VA and ICA was performed using Pearson correlation analysis. There was no statistically significant correlation between sum of bilateral VA, ICA and CBFV with age in both groups (r=0.11, p=0.56; r=0.61, p=0.75; r=0.91, p=0.63 in PCOS group and r=0.41, p=0.076; r=0.37, p=0.11; r=0.29, p=0.22 in control group, respectively). DISCUSSION The significance of PCOS derives from a range of endocrine and metabolic abnormalities, in which insulin resistance is at the center. The vascular dysfunction in PCOS was also hypothesized to be caused by insulin resistance (1,11,13-17). Kelly et al. (1) demonstrated impaired macrovascular and microvascular functions in women with PCOS when compared with a age matched control group of subjects. Despite these evidences of vascular dysfunctions in PCOS, we were unable to demonstrate any abnormal flow volume, RI and PI measurements of ICA and VA in patients with PCOS. It was reported that elevated androgen levels and insulin resistance in patients with PCOS appears to be associated with endothelial dysfunction and reduced endothelium-dependent vasodilatation (1,18). In the literature, there are many different conclusions about hemodynamic changes in patients with PCOS. Lakhani et al. (7) reported a decrease in ICA PI in patients with PCOS and they stated that lower PI with similar peak systolic velocity indicate reduced vascular resistance and increased blood flow. Controversially they also stated that in type II (non-insulin-dependent) diabetes, a condition which is closely related to PCOS, regional cerebral blood flow may be reduced. In another study, Battaglia et al. (9) reported decreased ovarian artery resistance and increased uterine artery resistance in patients with PCOS. In our study, we could not find any statistically significant difference between ICA PI values of patients with PCOS and control group. Furthermore, there was no significant difference in VA RI and PI values of both groups. This may have been resulted from parity characteristics or young age of the patients. It is well known that hormonal alterations have effects on pulsatility index however these changes takes time to be apparent (19). Therefore, we suggest that the probable changes of Doppler parameters in PCOS patients may be more significant with aging. To our knowledge, this is the first study in which CBF volume has been assessed using color duplex sonography in women with PCOS, and the results demonstrated normal CBF volume when compared with age-matched healthy controls. Our results for CBF volume were also in substantial agreement with those published previously for young women with CBF volume of 730±87 mL/min (20). Most publications dealing with CBF measurements in healthy adults report a decline in CBF with increasing age, mainly due to a reduction of cortical blood flow while only few authors found that global CBF remains constant during healthy normal aging (20,21) It has been also reported that while ICA flow decreases with age, VA flow shows no change (21,22). In the present study, there was no statistically significant correlation between VA, ICA and CBF volumes with age in both groups. Absence of elderly women in PCOS and control groups might have caused this result. In our study, the mean VA velocity in patients with PCOS was significantly lower than control group (p=0.018). We could not find any physiological explanation for the mechanism responsible for decrease in VA velocity in patients with PCOS. Although VA velocities were lower in PCOS patients, there was no statistically significant difference between VA flow volumes. This indicates that differences of velocities are compensated by the diameter changes of VA. Consequently, the flow volume of posterior circulation does not change considerably. PCOS patients do not seem to have significant hemodynamic changes since their VA, ICA and CBF flow volumes were in normal limits when compared with control group. The absence of significant hemodynamic changes in our patients may be resulting from their considerably young age and relatively narrow age range. Therefore we think a further study including elder women is necessary to make clear this issue. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}
{kind=link}