 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 3, 2005, pp. 96-99 EXPERIENCE OF AMBULATORY LAPAROSCOPIC CHOLECYSTECTOMY IN TURKISH PATIENTS İbrahim Barut, Ömer Rıdvan Tarhan , Celal Çerçi, Mahmut Bülbül Suleyman Demirel University, Faculty of Medicine, Department of General Surgery,
Isparta, Turkey Code Number: gm05021 Aim: Laparoscopic cholecystectomy (LC) has become established
as the standard procedure for gallstone disease. This study was performed to
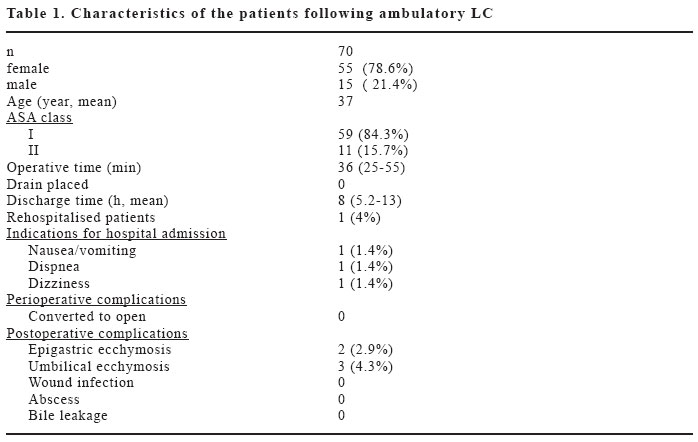
investigate safety and efficacy of ambulatory LC in selected patient population. Key words: Ambulatory, Outpatient, Laparoscopic cholecystectomy. INTRODUCTION Surgical removal of the gallbladder for symptomatic gallstones is an established operation that was first performed in 1882 by Carl Langenbuch (1). Since the introduction of laparoscopic approach a decade ago, surgeons and patients have lowered the threshold for proceeding to cholecystectomy (1). Laparoscopic Cholecystectomy (LC) has received near universal acceptance and is currently considered the "gold standard" for treatment of cholelithiasis (2-6). The main advantages of this technique are earlier return of bowel function, less postoperative pain, shorter duration of hospitalization, more rapid return to full activity, and decreased overall costs (2-8). Ambulatory surgery is the oldest known form of surgery. Early discharge after operations does not increase the complication rate. It has been pointed out that morbidity begins in the operating room, not at home, and clinicians tend to be meticulous with a patient scheduled for early discharge to minimize complications (9). Ambulatory LC had not been performed for a long period with the fear of serious complications such as bleeding and fistula or other reasons for readmission, and the argument that patients might feel safer when observed for one night (3, 10-13). But the advantages of LC has encouraged performing this technique as an ambulatory procedure and it has become popular in all countries recently (3, 6, 11, 12). This study was performed to investigate the safety and efficacy of ambulatory LC in a carefully selected patient population without overnight stay in hospital. To the best of our knowledge this is the first report of ALC in English literature from Turkey. MATERIAL AND METHODS A total of 70 patients were included the study in General Surgery Clinics of Alanya Private "Hayat" Hospital, Çankırı State Hospital and Suleyman Demirel University School of Medicine between June 1999 to June 2004. Patients were selected for ambulatory LC based on The American Society of Anesthesiologists (ASA) classification (14) and the patient's willingness to accept the outpatient procedure. ASA-I and ASA-II patients were included into the study. There was symptomatic cholelithiasis in all patients. All the patients were undergone physical examination, routine biochemical and hematological analysis. Upper abdominal ultrasound was also performed routinely. The patients were evaluated by the clinics of anesthesiology and cardiology preoperatively and were hospitalized at the operation day. The patients were given 1 g. Ceftazidim (Fortum®, GlaxoSmithKline, Izmit, Turkey) via intravenous route an hour before the operation as an antibiotic prophylaxis. Nasogastric decompression was performed to all patients perioperatively and was removed at the completion of the procedure. The standard American technique was successfully used in all patients. The operating surgeon was not surgical resident, and used two-handed technique. The 10-mm trocar sites were closed. Pain control in the patients was provided with local anesthetic infiltration perioperatively (0.5% bupivacaine HCl about 5 cc. for each trocar sites), and with the usage of diclofenac sodium postoperatively for three days (as daily dose 75 mg). Ondansetron HCl was given to all patients for the possible symptoms of nausea and vomiting in the postoperative period (as single dose 4 mg). Patients were discharged when they were able to meet standard discharge criteria (adequate pain control, ability to stand, ambulate, void, and tolerate oral liquid), in case vital parameters and physical examination were normal and there were no subjective symptoms in the postoperative period. Patients were given instructions to contact their attending surgeon if they developed fever, chills, evidence of bile drainage from the incision, significant nausea and/or vomiting, or abdominal pain. The patients who discharged were called via telephone in the evening and asked about their subjective symptoms. Patients were also then followed up by telephone calls at 24 and 48 hours. All patients were seen postoperatively in 7 to 10 days for a follow-up examination. The results were evaluated to investigate the safety and efficacy of ambulatory LC in a carefully selected patient population without overnight stay in hospital. RESULTS Overall, 70 patients underwent elective LC (Comparison of the patients following ambulatory LC is shown in Table 1). Preoperative diagnosis was symptomatic cholelithiasis in all patients. The patient population consisted of 55 female (78.6%) and 15 male (21.4%) with an age range of 19 to 66 years (mean age 37 years). The American Society of Anesthesiologists (ASA) classification of the patients found that 59 of them (84.3%) were ASA-I, 11 patients (15.7%) were ASA-II. The duration of the operation was between 25 to 55 minutes (mean 36 minutes). No patients underwent conversion to an open cholecystectomy. Perioperative complications did not occur in any of the patient. No drain was used in all patients. All of the patients were discharged at early postoperative period (range 5.2-13 hours, mean 8 hours). Mean hospital stay was about 10 hours for the first 30 patients, and about 6 hours for the last 40 patients. Only one patient who had dyspnea, nausea, vomiting and dizziness was rehospitalised. The patient was in ASA-II classification (heavy smoker), and remained in the hospital for 24 hours. Symptomatic treatment was performed and he was discharged 24 hours after surgery uneventfully. In postoperative 7th day, ecchymosis at epigastric port and umbilical port sites was determined in 3 patients and 2 patients, respectively. These ecchymosis resorbed spontaneously. DISCUSSION Currently, LC is almost universally applied and is considered by most to be the "gold standard" for the treatment of symptomatic gallbladder disease (3). Ambulatory LC is becoming increasingly accepted as its safety and feasibility (4). This procedure significantly decrease duration of hospitalization and the average hospital cost (12). We found that ambulatory LC is safe and effective procedure for the carefully selected patients. Ambulatory LC is preferable for Turkish patients because staying at home is more comfortable. Telephone follow up of the patients seems as an effective follow up (3, 15, 16). We also observed that this approach causes a confident relationship between the surgeon and the patient. Widespread use of the LC as an ambulatory procedure will lead to increase all other ambulatory surgical procedures. Consequently, this approach will decrease the hospital costs and encourage establishing outpatient clinics in developing countries as Turkey. Postoperative pain, nausea and vomiting after laparoscopic cholecystectomy have been important limiting factors for ambulatory laparoscopic cholecystectomy (6, 17, 18). Perioperative infiltration of local anesthetic to the trocar site and postoperative parenteral analgesic and ondansetron application improve patient comfort and success of ALC (6, 19-21). Infiltration anesthesia to the trocar site and using ondansetron was found effective as in the series of some studies (6, 19, 20). We obtained that our results were compatible with these studies'. Characteristics of our study: 1.Patient population that was very carefully selected, 2.In addition to the standard American LC technique, local anesthetic application with bupivacaine administered to the trocar sites, 3.Telephone follow-up was performed by the surgeon, 4.The study was performed in all three kinds of hospitals namely state, private and teaching hospital. In the report by Robinson et al. (4), Serralta et al. (22), Hollington et al. (23), the readmission ratios were higher (50%, 23.6 %, 18.3%, respectively) than the present study (1.4%). It's thought that the high readmission ratios reported in these studies are associated with unselected patient population. Only ASA-I and ASA-II patients were included in our study and ALC was not performed to the ASA-III and ASA-IV patients. It has been suggested that selection of the patients (ASA-I and ASA-II) improved the success of ALC while decreasing readmission rate. It's also found that the telephone follow-up by the surgeon was effective. We observed that this method provided winning the patient's confidence. This study could not clarify the feasibility of the ALC in ASA-III and ASA-IV patients. Further studies are necessary for the evaluation of feasibility of ALC in ASA-III and ASA-IV patients. Despite the number of patients in the study were limited in 70 patients, the successful results of ALC encourage us to apply this procedure more widely, i.e. ASA-III and ASA-IV patients. In conclusion, ALC as true outpatient procedure can be routinely applied to selected patients at all medical centers. ALC is effective and safe procedure that can be recommended for carefully selected patient population without overnight stay in hospital. It has been suggested that selection of the patients (ASA-I and ASA-II) improved the success of ALC while decreasing readmission rate. Telephone follow up of the patients seems as an effective follow up. This approach will decrease the hospital costs and encourage establishing outpatient clinics in developing countries. Perioperative infiltration of local anesthetic to the trocar site and postoperative parenteral analgesic and ondansetron application improve patient comfort and success of ALC. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}