 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 3, 2005, pp.100-109 EFFECTS OF HIGH FAT DIET INDUCED OBESITY ON FEMALE RAT LIVERS (A HISTOCHEMICAL STUDY) Zuhal Altunkaynak Atatürk University, Faculty of Medicine, Department of
Histology and Embryology, Erzurum , Turkey Code Number: gm05022 Aim: Obesity is an important, complex and chronic disease.
Fatty diet is a significant factor causing obesity. It is known that obesity
is associated with many chronic disorders such as Non-Alcoholic Fatty Liver
Disease (NAFLD). However, mechanism of this event is yet unclear. In this study,
it was purposed to examine histological effects of fatty diet induced obesity
on liver from female obese rats. Key words: Liver, Light microscopy, Fatty diet, Obesity. INTRODUCTION Obesity is a severe metabolic disorder, characterized with increases in energy intake and a decrease in energy output concerning body weight and glucose metabolism (1) Obesity is associated with many important complications such as diabetes and coronary heart disease (2) sleep apnea and pulmonary dysfunction, stroke, diseases of the gallbladder, liver and the musculoskeletal system, reproductive dysfunction, venous insufficiency, deep vein thrombosis, poor wound healing, and more (3). Ramos et al. thought that obesity should be a low-grade inflammatory disease because most of the obese patients had shown increased levels of interleukin-6 and tumor necrosis factor-alpha, both markers of inflammation (4). Obesity may be the underlying reason of cancers of the breast, endometrium, colon and prostate. Obesity is an increasing problem in modern societies, due to the adoption of rapid lifestyle which results in high dietary intake of carbohydrates and fat accompanied by reduced energy consumption (2). More than half of adult Americans are overweight or obese, like populations of many other countries (2). Obesity is associated with insulin resistance and hyperlipidemia (5). In obese dogs, hyperinsulinemia and hepatic glucose deproduction are reported (5) and predominantly visceral adipose tissue increases accompany insulin resistance (6). A significant connection between non-alcoholic fatty liver disease and findings of insulin resistance has long been reported. Most cases of NAFLD occur in patients with obesity, type 2 diabetes mellitus and hyperlipidemia (7). NAFLD is one of the most common causes of chronic liver disease (8, 9). Obesity is an important risk factor in pathophysiology of NAFLD, cirrhosis-associated death (10) and liver cell cancer (11). In many cases NAFLD is histologically indistinguishable from alcoholic liver disease (12-16). Many NAFLD patients having liver fibrosis may be subject to cirrhosis and its complications (15-17). But the histological mechanism of NAFLD is unclear (18). In a previous study, it was observed that NAFLD patients have; significant lobular inflammation, hepatocellular necrosis, hepatocellular ballooning, portal tract inflammation, pericellular and portal fibrosis as described (19). In electron microscopical examining; enlargement of microvilli, arising in number of lysosome, cytoplasmic swelling etc. was reported (20). But procession of histological damage is unknown. In this study, four different histochemical methods were used for evaluation of the structure of liver light microscopically. Also livers collected from rats in different stages of experiment. Many previous studies performed on mice and rats suggested that obesity can be induced by high fat diet (21). Current study comprises usage of a diet-induced obesity model by proposing high fat diet on adult female rats and examination of the livers of these obese rats under light microscope. Thus, we tried to understand the effects of obesity on adult female liver. MATERIAL AND METHODS Animals; 20 adult female Sprague Dawley rats, weighing between 150-200 gr were used. All animals were obtained from the Ataturk University Study Applying and Research Center. The rats were maintained in laboratory under controlled environmental conditions (12 h light/ dark cycle and room temperature 22-240C and mated overnight. Rats were housed in plastic cages (two animals in per cage) and given food and water ad libitium. Diets; Standard diet is used under supervision of the animal care committee of the university. Control rats (n:8) were fed standard rat chow (7-10% fat, 68-70% CH, 18-20% protein, 1-2% vitamins and minerals; 210 kcal/100 gr/day). Later, isoenergic high fat induced diet is consist of 30% calories from animal fat (30% fat, 50-52% CH, 18-20% protein 1-2% vitamins and minerals; 210 kcal/100 gr/day), the diet was prepared and necessary vitamins and minerals are added. For fatty diet; the chow, in powder form, was mixed with added 30% melted animal abdominal fat until become homogenous in a dough-like consistency. This dough was shaped with a paste injector. Obtained chow blocks were dried and used for feeding. Study Design; All animals were randomly assigned into two groups as control and study groups. While control rats (n:8) were maintained on standard chow, the study group (n:16) were fed with the specially prepared chow. All animals' weight was measured every 10 day in order to determine any weight rise. In the end of this study, all animals were sacrificed by sevorane® (Abbott, Ultane; Canada). The study group was divided into three different treatment groups on basis of sacrificing schedule according to our previous laboratory observations and literature. First treatment group was sacrificed at 8th week after the onset of the study (n:5). Remaining treatment groups were sacrificed at 10th (n:5) and 12th. (n:6) weeks respectively. All animals' body weight and nasoanal length were recorded for indirect computation of body composition via the Lee obesity index method (22). Thus, the status of the animals as to being obese or not, were confirmed. Then, non-obese animals were excluded from treatment groups. Perfusion fixation method is performed on sacrificed animals, as reported previously (23). Livers were removed from obese rats and subjected to histochemical processes in order to examine them under light microscopy. Histochemical Estimation at Light Microscopic Level; All chemical solutions were obtained from Sigma Aldrich Company; Deutschland. All removed-livers were fixed in a formaldehyde solution (which consists of 10 ml formaldehyde, 90 ml distilled water) for a duration of 48-60 hours. After this, tissue samples were processed through ethyl alcohol and xylene series, and embedded in paraffine blocks. Four histochemical staining methods were applied to the sections obtained from liver blocks. These methods are as follows:
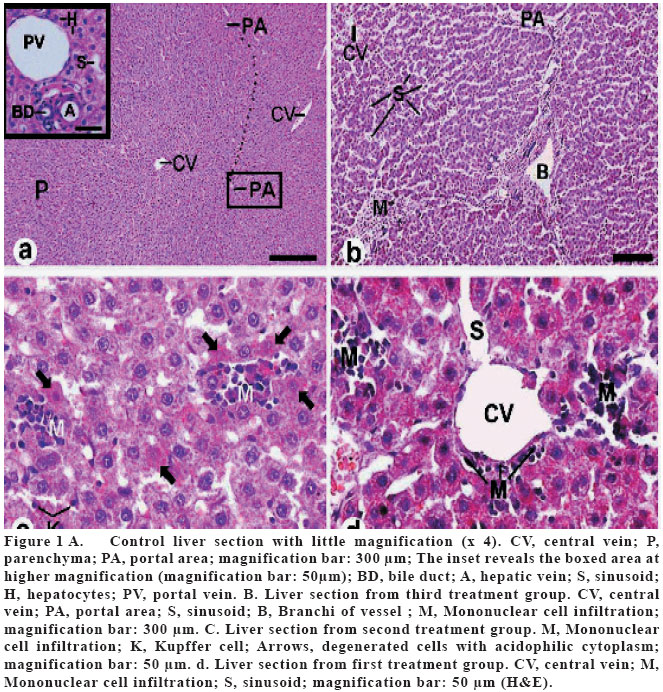
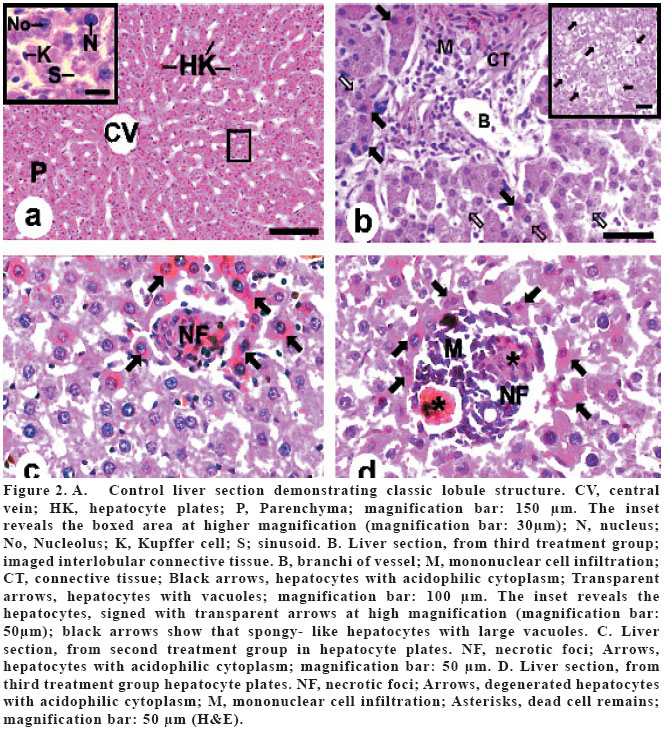
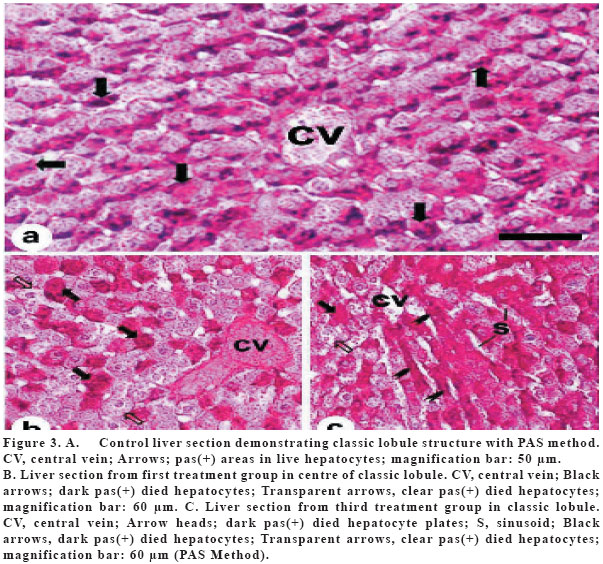
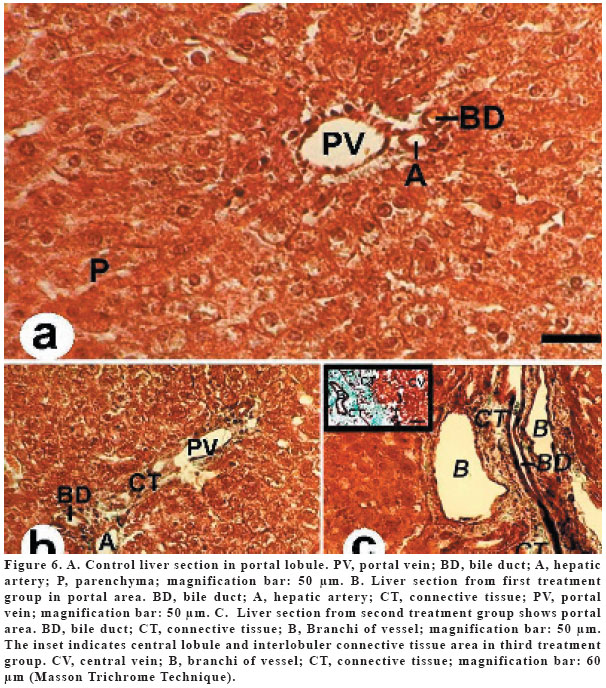
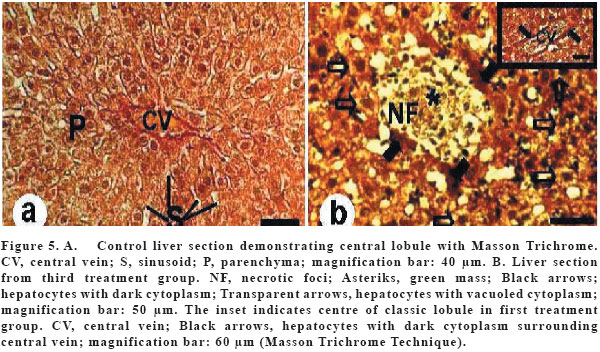
RESULTS There was no death of animal in the experimental period. In this study; two groups were used for histological assessment. These groups were control and study groups. Lee obesity index of both groups were 3,2 ± 0,3 kg/m2 (of control group) and 5,6 ± 0,5 kg/m2 (of treatment group). Study group was divided into 3 different treatment groups. Groups were randomly composed with treated animals. The first group was sacrificed on 8th week of the study. The others were sacrificed on 10th and 12th weeks respectively. Four histological methods were performed on all liver samples in order to be able to discern different tissue particles. Finally, all slides were observed under light microscope. At first, all slides were stained with Hematoxyline-eosin; to define routine histological structures. In control group; the central vein, the initial branch of hepatic vein, was occupying the longitudinal axis of each classical lobule (Figure 1a, 2a). Hepatocytes radiate, like spokes of a wheel, from the central vein, forming anatomizing, fenestrated plates of liver cells, separated from each other by large vascular spaces known as hepatic sinusoids (Figure 2a). The portal areas were isolated from the liver parenchyma by the limiting plate (Figure 1a). Resident macrophages, known as Kupffer cells were associated with the sinusoidal lining cells in the sinusoids (Figure 2a). In all study groups' sinusoids; central veins and branches of portal vein were dilated (Figure 1b, 1d). Significant mononuclear cell infiltration was observed both between the cell plates and around the dilated vessels (Figure 1b-c-d, 2b-d). These infiltration areas were enlarging progressively from 8th week (Figure 1d) to 12th week (Figure 1c, 1b, 2d, 2b). Also in study groups, some hepatocytes were more acidophilic than control group and there was cytoplasmic shrinkage and more dark and small nuclei in the acidophilic hepatocytes (Figure 1c, 2b, 2c, 2d). Moreover; many necrotic foci of progressive degrees were found from first treatment group to 3rd treatment group (Figure 2c, 2d). In the 3rd treatment group, these necrotic foci were surrounded by mononuclear infiltrative cells (Figure 2c, 2d). Especially in portal area of third treatment group's livers; not only dark acidophilic cells, but hepatocytes were also containing unstained cytoplasm and little vacuoles (Figure 2b). When slides stained with periodic acid- Schiff (PAS) method were examined, our first finding was; PAS (+) granules in apical cytoplasm were absent in study rats (Figure 3a, 3b). Study group hepatocytes were containing irregularly located PAS (+) granules and some hepatocytes were stained densely with PAS (Figure 3b, 3c). In study groups' slides treated with Oil Red O dye, more red drops were defined in a pattern increasing from first to 3rd treatment groups (Figure 4b, 4c, 4d). According to Masson's Trichrome Method, there appeared more green colored areas in the portal area of the livers of the study group than control group (Figure 6a, 6b, 6c). However; necrotic foci, which were previously observed by hematoxyline-eosin stain, were confirmed with Masson's Trichrome Method too (Figure 5b). But there was a green mass in the middle of these necrotic foci, especially in 3rd treatment group (Figure 5b). DISCUSSION Liver steatosis is a well-known pathology in severely obese patients and is especially associated with visceral adiposity and diabetes (18). It may progress in some patients to steatohepatitis and cryptogenic cirrhosis (18). The histological mechanism of non alcoholic fatty liver disease (NAFLD) is yet not understood (18). In many of obese people, increase of hepatic triglyceride levels, causes hepatic steatosis (24). The aim of this study was to investigate the effects of high fat diet (30%) on NAFLD histologically, in order to achieve this objective, obese rat model was constituted by means of fatty diet administration. Before this study, many articles were reported pertaining to this subject. Some researchers suggest that high fat diet causes abnormal mitochondria and mononuclear inflammation (25). It was claimed that lobular inflammation, pericellular fibrosis, portal fibrosis, hepatocellular ballooning, occures in consequence of oxidant stress and mitochondrial dysfunction in NAFLD (26). In a different study; we reported that enlargement of microvilli, balonning degeneration in hepatocyte cytoplasm and mytocondrial degeneration occurred in liver of obese rats (20). Current study indicated mononuclear cell infiltration, portal fibrosis, microvesicular fat globules and reduced glycogen content (27) in study groups' slides and orientation of hepatocyte plates was corrupted. This event may have occurred as a result of oxidative damage in hepatocellular proteins, Abraham P.et al. have mentioned the same in their study (28) or necrotic changes in hepatocytes. We determined that necrotic foci were progressed towards the end of the study. We found that vascular dilatation was gradually increasing, in both sinusoids and large vessels, light microscopically. As proved in this study, we are suggesting that feeding with fatty diet causes vascular dilatation, to our knowledge this finding was not reported before in the English literature. In our opinion; the progressive increase in the dilatation level during the course of the experiment, was due to the continuous effect of fat-rich feeding. We detected mononuclear cell infiltrations in both between hepatocyte plates and in around dilated vessels. About underlying reason of this condition some researchers claim this inflammation area, either in foci or diffuse form, occurs due to cytokine release resulting from fatty feeding (29). Besides, some researchers suggest that inflammation occurs as a response to hepatocyte damage (30). Also these researchers observed mixed inflammation cells in lobular parenchyma.(19, 31). But we observed only mononuclear cells in inflammation areas. We thought that these mononuclear cell infiltrations especially in portal area, indicated chronic inflammation in lobules and around the vessels. In our opinion, the reason of these focal infiltrations, in animals being fed by fatty diets would be the fatty content of the blood incoming to liver which first passes from portal area. Therefore, it was a predictable result that, fatty degeneration would first be detected in portal area. Moreover, this degeneration may point that liver damage could widen from around of lobules towards central area. But MacDonald et al. reported that degeneration first begins in hepatocytes of third zone (32). In this study, there appeared green areas with Masson's Trichrom Technique. Light green dye, which is used in this technique, stains collagen fibrils of connective tissue in green. Stellate cells, known as fat-storing cells, are perisinusoidal non-parenchymal cells which in normal liver are non-proliferative and are the main storage site for vitamin A. They contribute to fibrotic response following a process known as "activation", which induces the transformation of a resting perisinusoidal cell into one that is proliferative, fibrogenic and contractile. We spotted by this technique that connective tissue was increasing particularly in portal area and there was green material in necrotic foci. We observed many hepatocytes with dark basophil nuclei and acidophil cytoplasm around the necrotic foci would be involved in the necrotic process. In this study, these decreases in CH contents of hepatocytes were determined mostly by Periodic Acid Schiff (PAS) method. Further more, there were no hepatocytes with dark, PAS (+) stained cytoplasm. Oil Red O stain is used for detecting neutral fat content. Neutral fat vesicles are seen as red droplets with this dye. When study groups' livers were examined with Oil Red O stain, microvesicular steatosis is detected in granular cytoplasmic form. However, Duvnjak M, Virovic L. has reported a macrovesicular steatosis in a NAFLD patient's liver (33). Also, we found many hepatocytes with unstained granules by Hematoxylin-eosin in portal area. According to these results, our hypothesis is based on the finding that fatty degenerations begin in first zone (the closest area to portal triad) because this area subjects to toxic and hazardous material in blood, firstly. Then this degeneration widens towards the center of lobules and as a result fibrosis occurs as necrotic foci. Due to the structure and scope of this study, mechanism of fatty diet induced liver degeneration is not clearly understood. Although there are many studies about this subject in literature, in these studies; both diets were with high fatty percentage (%71) (25) and histological experiments were limited. Experimental diet, used in this study, was isocaloric with control diet. Also all animals were fed equal portion chow (210 kcal/100gr/Animal/Day). But in previous experimental studies, hypercalorical diets were used (1, 30). There was many experimental studies in literature about fatty diet induced obesity and these studies have different durations. In this study; we defined the duration of treatment as 8, 10 and 12 weeks, respectively to detect histological changes in a time dependent manner. We conclude that previous findings may be the result of high calories. However, our findings indicate an absolute fatty effect. Also we detected important histological features such as microvesicular steatosis, mononuclear cell infiltration and fibrosis as necrotic foci. We had the chance to examine the course of liver damage closely. In the literature many researcher applied an obesity model with fatty diet during different time.1,5,10,21,27 such as 8 week, 16 week, 28 day etc. According to literature and our previous laboratory experiences, we planned this study as 3 different stages (8th., 10th., 12th weeks). Therefore, In this study, of which %30 fatty diet was used, we are suggesting that fatty diet is the main cause of hepatocellular necrosis formation on liver (due to free radicals or oxidative damage). Vascular dilatation, inflammation and fibrosis outcomes were determined following this formation. Acknowledges: I am greateful to my advisor Assoc. Prof Elvan Özbek. MD. for his important academical contribution. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}