 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 3, 2005, pp. 110-113 ETIOLOGY AND PROGNOSIS IN 36 ACUTE RENAL FAILURE CASES RELATED TO PREGNANCY IN CENTRAL ANATOLIA Lütfullah Altıntepe1, Kazım Gezginç2, H. Zeki Tonbul1, Çetin Çelik2, İbrahim Güney1, S. Tülin Gezginç2, Süleyman Türk1 Selçuk University, Faculty of Medicine, Departments of Nephrology Division1 and Obstetrics and Gynecology2, Konya, Turkey. Code Number: gm05023
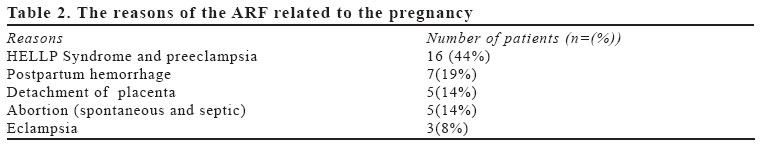
Aim: In this study, the reason of the acute renal failure (ARF) clinic features and results of it has examined as retrospectively. Key words: Pregnancy, acute renal failure, prognosis. INTRODUCTION In the developed countries decrease in ARF incidence occured because of the legality of the abortion and the developments in the antenatal care. There had been a difference between the developed and undeveloped countries about the frequency and the etiology of the ARF because of some environmental and socioeconomic reasons (1-3). In the developed countries, before the years 1960-1970 all the ARF cases in women were related to the pregnancy and the ratio was 40-50%, and this was effecting the 1/2000-5000 of the all pregnancies. Today this ratio has decreased to 5% and 1/10000. In the third world countries still pregnancy causes 25% of the ARFs. This situation causes high risk for maternal mortality (9-55%) (4-8). All the factors that can cause ARF in a non-pregnant woman can cause theoretically ARF in a pregnant woman. Even if the placenta detachment and preeclampsia is known as the most common reason of the ARF related to the pregnancy associated acute renal failure has now, all the factors that are related to the pregnancy has now been multifactorial because of the improvements in the antenatal care and early diagnosis of pregnancy complications (9). The abortion induction incidence for unwanted pregnancies is very rare in the developed countries, but in the developing countries it is still high (10). In this study, in 36 cases who were examined for Acute Renal Failure (ARF) between the years 1997-2001, the reason of the ARF, clinic features and outcome was evaluated retrospectively. MATERIAL AND METHODS Between 1997 and 2001, among 283 ARF cases followed up by our clinic, 36 cases (12.7%) were associated with pregnancy, the reason of the ARF, clinic features and outcome were examined retrospectively. Ages of patients, number of the pregnancies, history of chronic hypertension and prior births were registered. The medical history of the patient, physical examination, routine urine analysis, BUN, serum creatinin, urine creatinin and fractional sodium extraction, renal ultrasonography and selective renal angiography (when necessary) were examined. The progressive increase in the level of the serum creatinin with or without oliguria was accepted as ARF. The daily urine output less than 400 ml was accepted as oliguria. The cases who had a past history of renal illness. The medical history of the patient, physical examination, routine urine analysis, BUN, serum creatinin, urine creatinin and fractional sodium extraction, renal ultrasonography and selective renal angiography were examined and diagnosed the ARF with these. The progressive increase in the level of the serum creatinin together with the oligoanüria was accepted as ARF. The daily urine output less than 400ml was accepted as oliguria. The cases who had a past history of renal illness were not included in this study. The HELLP syndrome was established with physical examination (icterus, arterial hypertension), peripheral spread, serum total and direct bilirubin, reticulocyte count, urobilinogen in the urine, serum lactate dehydrogenase (LDH), AST, ALT, and platelet counts The presences of hemolysis (indirect bilurubin >1.2 mgr/dl, LDH > 600 U/L), elevated liver enzymes (AST> 70 U/L) and trombocytopenia (< 100 000/mm3) were accepted as HELLP Syndrome (11). Apgar score and birth weight of babies were registered. Applied treatment, complications and results of pregnancy were determined. The prognosis of the patients were evaluated as; complete improvement, partial improvement, irreversible renal failure and dead. The complete improvement in the renal functions was accepted as complete recovery. The decrease of the level of serum creatinin under 2mg/dl, normal urine output and lack of need for hemodialysis was evaluated as partial recovery. But the continuing need for dialysis was defined as irreversible renal failure. The data were analyzed by using SPSS for Windows 9.0 statistics package. The results of the patients were given as median ± standard deviation. Chi square and Fisher's Exact tests were used in statistical analyses. P <0.05 was accepted as the level of statistical significance. RESULTS ARF were developed related to the gestational problems in 36 of the ARF patients (12.7%). Avarage of the pregnancy; below 20 years old patients was 1, between 20-29 years old patients, 9, between 30-40 year olds 22 and over 40 years old 4. Most of the pregnants with ARF were (61.1%) between the ages 30-40. The ARF related to the pregnancy were shown in the Table 2. The ARF related to the abortion has developed in 3 cases in first trimester and in 2 cases in second trimester. The number of pregnancy in cases with ARF; 4 cases in the first pregnancy (11%), 8 cases in the second pregnancy (22%), and 24 cases in third or the other pregnancies (67%). The symptoms and the findings at the time of admission of the ARF patients were shown in Table 3. All cases had oliguria and the average of the oliguric period was 4.8±8.7 (2-27) days and the staying period in the hospital was 11.7±7.6 (4-28)days. The laboratory values at the time of admission of the ARF patients were shown in Table 4. In 8 cases (22%) hyperpotasemia, (> 5.5meq/dl), in 12 cases (33%) anemia (<10 gr/L) and in 21 cases(58%) hypoalbuminemia (<3 gr/dl) were detected. Pregnancies were terminated. by Ceserean section In 15 cases (48%), by induction in 16 cases (52%). The avarage of Apgar score was 5.4±2.7 (0-8) and the avarage of birth weight was 1570±727 (300-3400) g. In the 9 cases there were intrauterine dead fetuses (25%). There had been antenatal dead in 3 cases. In 2 cases septic shock, in 3 cases disseminated intravasculer coagulation (DIC), in 4 cases Adult Respiratory Distress Syndrome (ARDS) and pulmonary edema, in 1 case puerperal infection, in 1 case acute cortical necrosis and in 3 cases gastrointestinal bleeding developed. Hemodialysis was applied to 17 cases (47%), only medical treatment applied to 19 cases (53%). 32 cases were improved completely (89%). 3 cases (%8) died because of multi organ failure (DIC and septic shock, DIC and gastrointestinal bleeding and ARDS). One case has taken to regular hemodialysis program because of cortical necrosis. (Table 1) DISCUSSION The incidence of ARF related to pregnancy in the developed countries was 1-2.8%, in the developing countries that was 9-25%. The reason of the lower incidence in the developed countries is the prevention of the pregnancy complications and early treatment, and more effective treatment of the preeclampsia. Septic abortion is no more seen in developed countries.(12, 13). In the middle of the 1970s, the main reason of the ARF in our country was related to the pregnancy related ARF (4). Utas et al compared the reason and the frequency of the ARF between the sessions 1983-1990 (116 ARF patients), and 1991-1997 (323 patients), and they reported reduction of the obstetric reasons ( 19% vs 14.9% respectively) (14). Selcuk et al evaluated the prevalence of the ARF related to pregnancy among 487 ARF patients in 3 different periods; 1980-85: 27/155 (17.4%), 1985-89:17/110 (15.4%), 1989-97: 30/220 (13.5%) (χ2=1.08, p>0.5) (5). Similarly, in our study the ARF frequency related to the pregnancy was detected as 12.7%. But, this rate was higher than the results in the developed countries. Utas et al reported that etiology of the ARF related to the pregnancy (n=70) were as follows; eclampsia (50%), HELLP Syndrome (15.7%), postpartum hemorrhage (14.3%), septic abortion (11.4%) and postpartum ARF (8.6%) (14). Selcuk et al, on the other hand, reported etiology of the ARF related to the pregnancy as follows (n:74); Abortion (30%), HELLP Syndrome and preeclampsia (14%), preeclampsia or eclampsia (12%), postpartum hemorrhage (15%), fetal dead (12%), decolman placenta (6%), placenta previa (1%) (5). In contrary to these studies; we detected that eclampsia and abortion in etiology is in a less frequency. In our study the HELLP Syndrome was the foremost reason. In our country the rate of ARF related to the septic abortion had reduced from 33.3% to 1.8% in the last 20 years. The improvement in the socioeconomic situation, early diagnosis and treatment of the complications related to the pregnancy and the legality of abortion had helped this improvement (5, 14-15). Selcuk et al detected that the rate of septic abortion as the reason of the ARF reduced. It was 33.3% in 1980-85, and reduced to 6.3% in 1989-97 (5). Utas et al reported that there had been an reduction in the septic abortion rate when we came to 1991-97 (8.3%) from 1983-90 (18.2%) (14). Vladitiu et al, from Romania had reported that after the legalization of the abortion in Romania in 1989 the septic abortion rates reduced from 20.6% to 1.5% (16). In our study the septic abortion frequency was detected as 2.6%, which is very less. Utas et al detected that the maternal mortality reduced to 20.8% in 1991-97 when compared to 31.8% in 1983-90 (14). Selçuk et al, on the other hand detected the maternal mortality as 18%. In this study it is reported that the main reason of the dead is septic shock (61%). The fetal dead was 9 (12%) (5). In our study the rate of the maternal mortality was lower (8%) but, this rate was higher compared to the developed countries. As a result, the ARF related to the pregnancy was seen commonly in the third or the other pregnancies and the most common reason was HELLP Syndrome, placenta detachment, and postpartum hemorrhage and it caused a high risk for fetal and maternal mortality. Therefore, we think that the number of the pregnancies should be limited and especially multipar pregnancies must be closely controlled for the prevention of pregnancy related ARF. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}
{kind=link}
{kind=link}
{kind=link}