 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
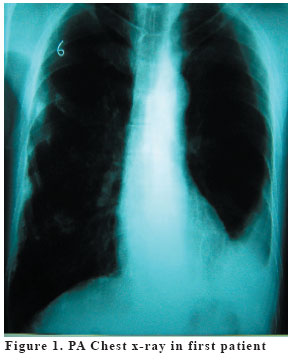
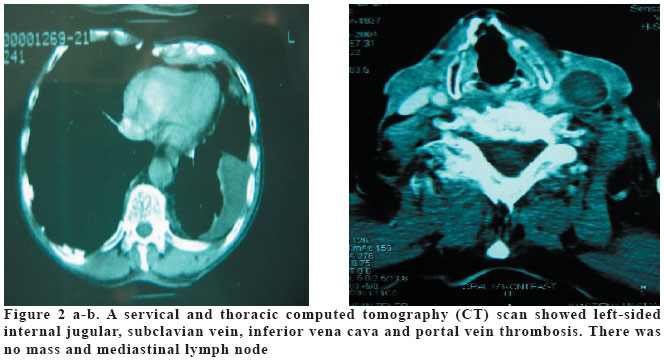
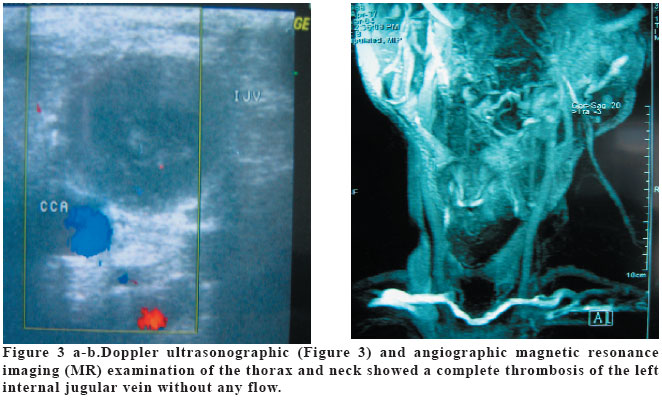
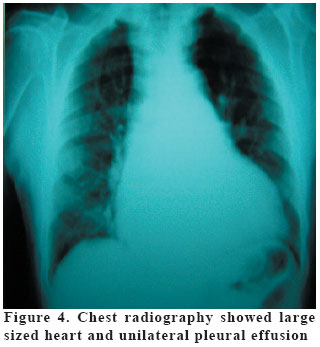
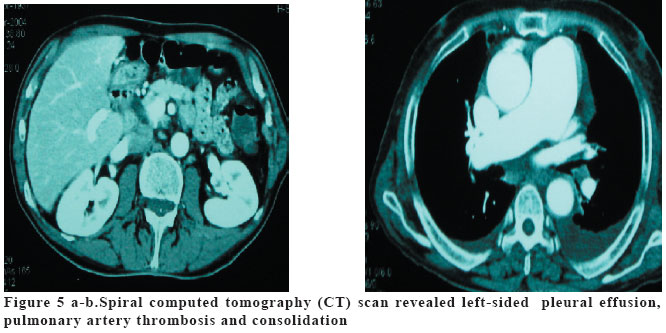
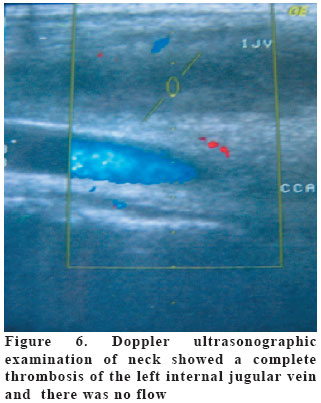
European Journal of General Medicine, Vol. 2, No. 3, 2005, pp. 123-128 INTERNAL JUGULAR VEIN THROMBOSI TWO DIFFERENT ETIOLOGIES Reha Erkoç1, Kürşat Uzun2 Köksal Yuca 3, Ömer Etlik4, Ekrem Doğan1, Hayriye Sayarlıoğlu1, Ayten İşlek2, Hakan Çankaya3 Yüzüncü Yıl University, Medical School, Departments of Internal Medicine1, Pulmonary Diseases2, Otorhinolaryngology3, and Radiology4 Code Number: gm05026 Internal Jugular vein (IJV) thrombosis is a rare entity. It is usually secondary to various etiologies such as catheter, malignancy, trauma, infection and hypercoagulable status. Associated malignancies, either known or occult, are also uncommon and not well documented in the etiology of IJV thrombosis. We reported IJV thrombosis with two different pathologies i.e. malignacy and congestive heart failure. The diagnosis of IJV thrombosis was established with Doppler ultrasound and CT scan. These patients were treated low-molecular-weight heparin and oral anticoagulation. Early diagnosis and appropriate management is important to prevent potentially fatal complications from internal jugular vein thrombosis. Key words: jugular vein, thrombosis, malignancy, heart failure INTRODUCTION Thrombosis of the internal jugular vein is a relatively rare condition. It is generally associated with central venous catheterization, neck surgery, trauma, endocrine alterations, coagulation disorders, hypercoagulable states, local infection or malignancy (1-3). Head and neck vein thrombosis without any obvious cause may be the initial manifestation of an occult malignancy (4). Internal jugular vein thrombosis presents with pain and swelling of the face and presentation may at times be subtle (5). Regardless of the cause, the role of the computed tomography, Doopler ultrasound and Magnetic Resonance imaging have been well described for the diagnosis of the IJV thrombosis (6, 7). We reported the radiologic and clinical findings in two cases with jugular thrombosis. CASE 1 A 67-year-old man presented with a one month history of left-sided chest pain and swelling of the left side of the neck. There was no other symptom. His medical history revealed heavy smoker (one packet of cigarettes per day for 50 years). Examination of his neck showed swelling on left side of neck. On physical examination, there were decreased respiratory sounds, and vibration thoracic and dulness on percussion on left thorax, heart examination was normal. There was no palpable cervical, axillary or inguinal lymph node. Body temperature was 37.2 oC, pulse was 75/min, and the respirations were 18/min. The blood pressure was 120/70 mmHg. Chest radiography showed a normal sized heart, left-sided pleural effusion and bilateral pleural calcifications (Figure 1). A servical and thoracic computed tomography (CT) scan showed left-sided internal jugular, subclavian vein, inferior vena cava and portal vein thrombosis. There was no mass and mediastinal lymph node (Figure 2 a-b). Doppler ultrasonographic (Figure 3) and angiographic magnetic resonance imaging (MR) examination of the thorax and neck showed a complete thrombosis of the left internal jugular vein without any flow. Haemoglobin value was 13 g/dl, white cell blood was 10000/mm3. Erythrocyte sedimentation rate (ESR) was 73/ hour, D-dimer was 2.47μg/ml. Tumor markers in serum were as follows; CA15-3 was 225 U/ml and CA 125 was 25.6 U/ml. Transthoracic echocardiography showed normal findings. Serum levels of antitrombin III, protein S and protein C were normal. Antinuclear antibodies, anti-DNA antibodies, anti neutrophil cytoplasmic antibodies, antiglomerular basal membrane antibodies, serum IgG and IgM anticardiolipin antibodies and rheumatoid factor were negative. Cytology of pleural fluid revealed adenocancer. Bronchoscopy was normal. Heparin was given by the intravenous route in therapeutic doses and then oral warfarin treatment was given. After anticoagulant therapy, a Doppler ultrasound and CT showed no recanalization of the internal jugular vein. CASE 2 A 81-year-old woman was admitted to the hospital because of congestive heart failure, shortness of breath at rest, cough, hemoptysis, chest pain, and swelling of the left upper extremity and left side of the neck. On admission, temperature was 37oC, pulse was 112 beats min-1 and respiratory rate was 22 min-1. Her blood pressure was 140/80 mmHg. Physcial examination revealed left-sided swelling of neck and left upper extremity. There were decreased movement of chest wall, decreased respiratory sounds, decreased vibration thoracic and dulness on percussion on left chest. Chest radiography showed large sized heart and unilateral pleural effusion (Figure 4). Spiral computed tomography (CT) scan revealed left-sided pleural effusion, pulmonary artery thrombosis and consolidation (Figure 5). Transthoracic echocardiography showed right ventricular hypertrophy and sistolic dysfunction of left ventricule. Pulmonary artery pressure was 70 mmHg, ejection fraction was 40%. No intraventriculer or atrial trombus could be detected. Doppler ultrasonographic examination of neck showed a complete thrombosis of the left internal jugular vein and there was no flow (Figure 6). Serum levels of antitrombin III, protein S and protein C were normal. Antinuclear antibodies, anti-DNA antibodies, anti neutrophil cytoplasmic antibodies, antiglomerular basal membrane antibodies, serum IgG and IgM anticardiolipin antibodies and rheumatoid factor were negative. Haemoglobin value was 12.3 g/dl, white cell count was 16300/mm3. ESR was 9/hour. Heparin was given by the intravenous route in therapeutic doses and then diuretic and digoxine therapy was performed. But, the patient died on 15th day of hospitalization due to cardiopulmonary failure. DISCUSSION Although less common than lower-extremity DVT, the incidence of DVT involving the upper extremities may be increasing and accounts for approximately 4% of all DVTs The most common predisposing factor is the presence of a central venous catheter, which is present in up to 75% of patients with upper extremity DVT (8). Marie et al. (9) reported that jugular vein thrombosis was 24.5% present in upper extremity deep venous thrombosis cases. In Marie's study, causative factors were malignancy (32.7%), venous catheters (22.4%) and thrombophilic states (8.2%). Marinella et al. (10) reported that etiology of upper extremity deep venous thrombosis were a central venous catheter in 72%, infection in 28%, extrathoracic malignancy in 22%, thoracic malignancy in 21%, renal failure in 21% and congestive heart failure in 8%. In Marinella's study, the left subclavian vein was involved in 49% of the cases. The association of cancer and thrombophlebitis was first observed by Trousseeau (11) and this association still bears his name. The incidence of thrombophlebitis in cancer patients is quite common and migratory thrombophlebitis is well documented. Reccurrent deep venous thrombosis, warfarin resistance, and thrombosis at unusual sites should increase suspicion of occult malignancy. The greatest risk of migratory thrombophlebitis is with pancreatic cancer; however it may be seen in a variety of adenocarcinomas, including breast, ovarian, and prostate cancer (11-13). A consistent observation is the low prevalence of concomitant cancer in patients with secondary thrombosis comparable to the prevalence in the general population. A 3 to19-fold increase in prevalence of concomitant cancer has been reported in patients presenting with an idiopathic venous thromboembolism (VTE). The prevalence of occult cancer in patients with secondary VTE is comparable with the prevalence of cancer in the general population, while the prevalence of occult cancer in patients with idiopathic VTE is 4-10% (14). In patients presenting with VTE, the prevalence of concomitant cancer, defined as cancer not known before VTE and discovered by routine investigation, varies considerably between the studies (14). This variation might relate to the depth of the routine examination, the variability of definition used for secondary thrombosis and differences in threshold of suspicion. It seems that some of the differences can also be explained by the age of the patients (15, 16). About 10-20% of the patients with VTE suffer from a known cancer. In our first case, there was pleural effusion and there was no mass and lymphadenopathy in lung and mediastenium. We performed thorasentesis because of pleural effusion. The diagnosis of pleural fluid was adenocarcinoma. Smoking has been shown to damage vascular endothelium, promote vascular thrombosis, and increase the relative risk of venous thromboembolism (17). Hansson et al (17) reported that smoking more than 15 cigarettes per day can increase the relative risk 2-fold over that of age-matched nonsmoking control subjects. In our report, only first patient was heavy smoker (50 pack-years) and the other patient was non-smoker. Venous thrombosis can result from disturbance of one or more pathophysiological mechanisms of play in Virchow's classic triad of endothelial damage, stasis and hypercoagulative state (18). A less common underlying condition for jugular vein thrombosis is congestive heart failure. Patients with heart failure may exhibit a low-flow state because of poor cardiac output, which may predispose to DVT (19). Bessoudo et al. (20) reported jugular vein thrombosis in a patient with congestive cardiomyopathy. In our second case, she had hypertension, chronic obstructive pulmonary diseases, chronic cor pulmonale, and systolic dysfunction. The most common symptom was pain, and the most common physical finding was edema in most studies (10, 21). Both of our patients had swelling on left side of neck as a tumor. There was no pain, edema and erythema. Accurate diagnosis of deep venous thrombosis is very difficult and imaging plays a crucial role in the diagnosis or exclusion of DVT. Although contrast venography is the gold standard for the demonstration of venous occlusion, there are many inherent risks of this modality. Noninvasive investigations, such as ultrasound, CT and MR, can establish the diagnosis of IJV thrombosis easily and have replaced the jugular venography, which carried significant risks, such as dislodgement of the clot and dissemination of septic emboli or trauma to the vein (18, 22). The initial test of choice for diagnosis of acute thigh as well as upper extremity DVT is ultrasound, because of its high accuracy, relatively low cost, portability, and lack of ionizing radiation. CT venography can be performed as a part of the examination. MR has a problem-solving role, and conventional venography is now limited to specific scenarious including evaluation of central DVT in the upper extremities (23). Accurate diagnosis chronic DVT remains problematic on all imaging modalities. Findings of chronic DVT include increased clot echogenicity, irregularly thickened venous walls, small caliber veins, and collateral veins. MR may reveal ancillary findings that may be contributing to the DVT. MR may be superior to US (24, 25). For both cases, patients had positive Doppler US that led to the diagnosis of internal jugular DVT. In addition, MR imaging and CT revealed internal jugular thrombosis. Reported complications associated with jugular vein thrombosis include septic emboli, pulmonary embolism, elevated intracranial pressure, facial edema, intracranial venous thrombosis and loss of vision (26). The incidence of pulmonary embolism after upper extremity DVT is approximately 14% (27). Second patient had pulmonary emboli. The treatment, although difficult, must be initiated with heparin; however, it is often unsuccessful and long-term therapy with either warfarin or heparin is typically not satisfactory. Patients with JVT may need to be on long-term oral anticoagulation therapy. Treatment of the underlying malignancy is the most definitive therapy, but usually in these particular diseases is also unsuccessful (28). We started low-weight molecular heparin for both cases, then, treatment was continued with oral anticoagulation. In first patient, resolution was not observed in spite of long-term anticoagulation, second patient died on 15th day of hospitalization. In conclusion IJV thrombosis is an uncommon and possibly life-threatening problem. IJV thrombosis can be occured in different pathologies. Early diagnosis and appropriate management is important to prevent potentially fatal complications from this condition. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}