 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 3, 2005, pp. 129-131 HYPERTROPHIC CARDIOMYOPATHY WITH MIDVENTRICULAR OBSTRUCTION IN ASSOCIATION WITH OSTIUM SECUNDUM-TYPE ATRIAL SEPTAL DEFECT Mustafa Aydın, Sait Mesut Doğan, Metin Gürsürer, Tolga Onuk Aydın Dursun, Fatih Cam Zonguldak Karaelmas University, Medical Faculty,
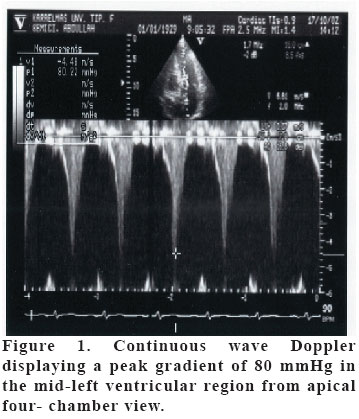
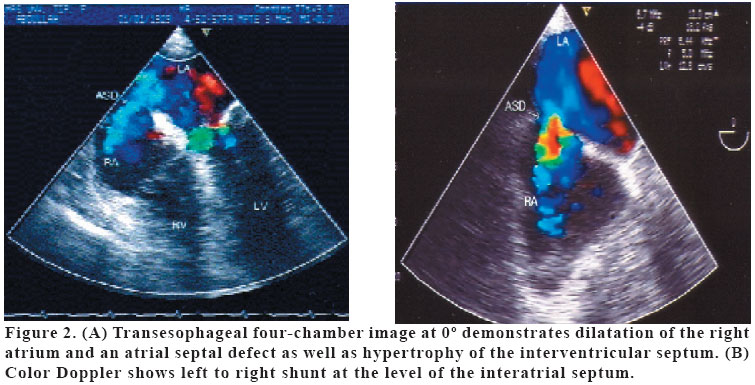
Department of Cardiology Zonguldak, Turkey Code Number: gm05027 This paper reports a 74 year-old-man with a hypertrophic cardiomyopathy associated with mid-ventricular obstruction and a secundum type atrial septal defect. He had been suffering from shortness of breath and occasional attacks of dizziness. Doppler echocardiography revealed the gradient in the mid-left ventricular area. A transesophageal echocardiogram confirmed the findings of transthoracic study and an ostium secundum-type atrial septal defect was documented. The present case represents a rare combination of hypertrophic cardiomyopathy associated with midventricular obstruction, and an ostium secundum type atrial septal defect in an elderly man. Key words: Hypertrophic cardiomyopathy, midventricular obstruction, atrial septal defect. INTRODUCTION Hypertrophic cardiomyopathy (HCM) is characterized by ventricular hypertrophy that is often asymetrical and associated with microscopic evidence of myocardial fiber disarray (1,2). The prevalance of this disease ranges from 0.02% to 0.2% (2,3). Its etiology is under debate; however it is now recognized that HCM may consist of heterogenous genetic diseases of the sarcomere (3,4). HCM has various manifestations with respect to the localization and extent of the hypertrophy (5). As we evaluate the types of HCM, the assymmetric septal hypertrophy is the most common type of HCM, the other forms of HCM including midventricular and apical are very rare. In some cases, left ventricular obstruction was present in the midventricular area, rather than left ventricular outflow tracts (6). Midventricular obstruction constituted only 1% of all cases of obstructive HCM (7). The association of hypertrophic cardiomyopathy with some isolated congenital anomalies of the heart have been reported, including pulmonary stenosis, corrected transposition of great vessels, and atrial septal defect (ASD). However, this type of HCM with midventricular obstruction together with ASD has been reported in very few case reports. CASE A 70-year-old man with a history of insulin dependent diabetes mellitus was examined for symptom of shortness of breath with moderate exercise and attacks of dizzeness on several occasions for the last two years. He did not have a family history of heart disease or sudden death. During the last three years, he presented with progressive deterioration of his functional class. In physical examination, auscultation revealed a II/VI systolic murmur along the lower left sternal border and pulmonary artery area, and a II/VI murmur was heard over the tricuspid area. The patient had a wide fixed S2 split. His blood pressure was 120/80 mmHg, the pulse rate was 74 beats/min, and rhythm was regular. The electrocardiogram demonstrated typical changes of left ventricular hypertrophy and strain. The transthoracic echocardiogram demonstrated left ventricular diameters within normal limits. Interventricular septal and posterior wall thickness measurements were 2 cm, and there was no paradoxical motion of the interventricular septum in parasternal long axis image with M-Mode echocardiography. The peak gradient registered in the mid-left ventricular area was 60 mmHg at rest without Valsalva maneuver. Systolic anterior movement of the mitral septal leaflet and left ventricular outflow tract obstruction were not documented. A Valsalva maneuver was performed and peak gradient of 80 mmHg was found in the mid-left ventricular region in Figure 1. Pharmacological challenge with nitrates was not attempted. Left ventricular relaxation was altered with diastolic relaxation abnormality as detected by an E/A ratio of 0.9, maximum velocity of the E wave was 1.1 m/sec and maximum velocity of the A wave was 1.3 m/sec. The isovolumetric relaxation time was prolonged (135msec). E wave deceleration time was 240 msec. The maximum velocity of the tricuspit E wave was 0.8 m/sec, and the maximum velocity of the mean pulmonary artery flow was 1.3 m/sec. There was mild dilatation of the right atrium and ventricle, and a moderate tricuspit regurgitation, from which pulmonary arterial systolic pressure was estimated to be 45 mmHg. A suspected view of ostium secundum-type ASD was obtained on transthoracic echocardiogram. Then a transesophageal echocardiogram was performed to confirm the findings of transthoracic echocardiogram, and an ostium secundum-type ASD was documented in Figure 2. Cardiac catheterization was not performed because the patient did not accept any invasive procedure. We chose a beta-1 selective beta-adrenergic blocker for the patient (metoprolol PO 50 mg/day) after confirmation of diagnosis for treatment of the intraventricular pressure gradient and the patient was taken under follow up. Frequency and severity of the symptoms decreased during a follow up of 6 months. DISCUSSION The present case is an elderly man of a hypertrophic cardiomyopathy associated with mid-ventricular obstruction and a secundum type ASD. HCM has been reported to have some different associations. In 1971, Forker et al. (8) reported a case of idiopathic hypertrophic subaortic stenosis and an ostium secundum type ASD. Hernandez-Reyes et al. (9) described a 36-year-old patient with nonobstructive septal hypertrophy and ostium secundum ASD demonstrated by transthoracic echocardiography and confirmed by transesophageal echocardiography of the septal defect. Long et al. (10) reported a case with association of ostium secundum type ASD and sinus venosus type ASD, as a very rare form. Smith et al. (11) defined a case with similar association in a patient who was later operated and ASD closure and septal myomectomy were performed. Branco et al. (12) reported a case with non-obstructive septal hypertrophy and ostium secundum type ASD who was diagnosed by transthoracic and transesophageal echocardiography and the diagnosis was confirmed by cardiac catheterization and the defect was closed surgically. In our case, the clinical symptoms could be related to left ventricular diastolic dysfunction as well as his hemodynamic status. The gradient in the midventricular area might lead to decrease in cardiac output, and then could cause those symptoms of the patient. Also dizziness which went on for a long time was thought to be related with an infrequent intervals of ventricular tachycardia, increase of midventricular obstruction with exercise and alterations in cerebral perfusion. Resolution of symptoms during follow up with metoprolol treatment in six months supports our idea. In such cases, normally, hemodynamic status is expected to be deteriorated, but in our case, preservation of hemodynamic status was thought to be due to small diameter of ASD. As the patient was old and pulmonary pressure was not so high, we were encouraged to follow the patient with medical treatment instead of surgical closure. As a result, we presented this case as it is a rare one, and there is no definitive treatment protocol for such cases. Whenever HCM is proved in a patient, as it is a congenital anomaly, it is important to keep in mind that another accompanied congenital defect could be present. REFERENCES
Copyright 2005 - Medical Investigations Society The following images related to this document are available:Photo images[gm05027f1.jpg] [gm05027f2.jpg] |
| |||||||||

{kind=link}
{kind=link}