 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
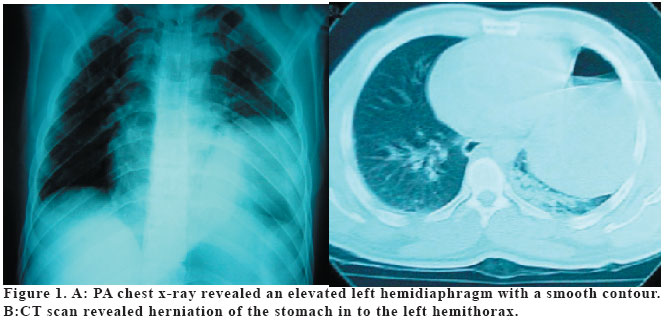
European Journal of General Medicine, Vol. 2, No. 3, 2005, pp. 132-134 TRAUMATIC ISOLATED PERICARDIO-DIAPHRAGMATIC RUPTURE Hıdır Esme1, Yusuf Yürümez2, Dursun Ali Şahin3, Osman San3 Afyon Kocatepe University, Faculty of Medicine, Departments of Thoracic Surgery1, Emergency Medicine2 and General Surgery3, Afyon, Turkey *Presented in Turkish Thoracic Society 8th Annual Congress, Antalya, Turkey. Correspondence: Hıdır Esme, M.D. Afyon Kocatepe University, Faculty of Medicine Department of Thoracic Surgery, Pembe Hastane, 03200, Afyon,Turkey Tel: 905336471729, Fax: 902722172029 E-mail:hesme@aku.edu.tr Code Number: gm05028 Pericardio-diaphragmatic rupture is an uncommon problem that poses a diagnostic challenge to surgeons. This article reports an unusual case of traumatic pericardio-diaphragmatic rupture in a 36-year-old male who has no additional intraabdominal visceral injury or thoracic pathology. There was a 7 cm lateral tear on the left dome of the diaphragm and a 2 cm medial tear, also involving pericardio-diaphragmatic junction, with the heart uninjured. The partially herniated stomach was easily pulled out from the thorax cavity through the diaphragmatic rupture. The rupture was reparied by interrupted non-absorbable sutures. The patient had no complaints on his follow up. Key words: Trauma, Pericardio-diaphragmatic rupture INTRODUCTION Traumatic diaphragmatic rupture (TDR) is not an uncommon injury, most noteworthy as a marker of severe trauma (1). The incidence of an additional injured viscera in diaphragmatic rupture is between 90% and 95% (2) . Pericardio-diaphragmatic rupture (PDR) is an uncommon problem that poses a diagnostic challenge to surgeons. The incidence of PDR is between 0.2% and 3.3% of cases with TDR (3) . We report an unusual case of traumatic PDR without additional visceral injury. CASE A 36-year-old male, road traffic accident patient was brought to the Emergency Department. The patient was complaining of left upper quadrant abdominal pain. Abdominal examination revealed epigastric abrasion, decreased bowel sounds, and diffuse moderate tenderness without rebound or rigidity. Auscultation of the chest revealed decreased breath sounds on the left lower and middle lung zones. There was no subcutaneous emphysema or any obvious rib or sternal fracture. Cardiac examination revealed a regular rate and rhythm without murmur, rub or gallop. Postero-anterior chest X-ray revealed an elevated left hemidiaphragm with a smooth contour made (Figure 1A). Left descubitus chest x-ray revealed air fluid level in thorax. The preoperative diagnosis of diaphragmatic rupture with probable partial stomach herniation was made in the emergency center based upon findings on the x-ray and Computed tomography (CT) scan of the chest (Figure 1B). An abdominal CT scan was negative for free fluid and hollow or solid organ injury. The patient was hemodynamically stable with no clinical evidence of pericardial tamponade. He was taken to the operating room two hours after trauma and thoracotomy was made. There was a 7-cm lateral tear on the left dome of the diaphragm and a 2-cm medial tear involving pericardio-diaphragmatic central rupture with the uninjured heart. The partial stomach was easily pulled out of the thorax cavity through a diaphragmatic rupture. The rupture was reparied by interrupted non-absorbable sutures. On the second post-operative day the patient had abdominal distention resistant to conservative treatment and consequently underwent explorative laparotomy in which no intra abdominal pathology was detected. Abdominal distention was referred to the chemical ileus secondary to bleeding which was caused by diaphragmatic rupture. The patient discharged on the ninth post-operative day and 3 months later he had no complaint on his follow up. DISCUSSION The first report of preoperative diagnosis of traumatic PDR appeared in 1951 (4). An average of only one report on a case of PDR is published annually. In 80% of the cases the cause is a motor vehicle accident, 17% are due to falls. The commonest location of the tear is the left pleuropericardium (62%) followed by the diaphragmatic portion of the pericardium (22%) (5). Right diaphragmatic rupture is encountered less frequently than left because of the buffering presence of the liver. The strong central tendon of the diaphragm is very rarely injured (3). In our case, the cause of the rupture was a motor vehicle accident and the tear was located in the diaphragmatic portion of the pericardium. PDR may mimic or present as pericardial tamponade, posing additional diagnostic and therapeutic difficulties. Herniation of visceral contents into the pericardial sac may produce acute tamponade, respiratory distress, or hypotension (3). Many investigative techniques have been described for the diagnosis of TDR, including chest X-ray, CT scan, magnetic resonance imaging (MRI), echocardiography, upper gastrointestinal (GI) contrast studies, angiography, ultrasonography, thoracoscopy, peritoneal lavage, and laparascopy (6). Chest X-ray is currently the most valuable simple test, although, it can be diagnostic or suggestive of TDR in only 28-70% of cases (7). The CT scan has been used increasingly to diagnose diaphragmatic rupture with or without a hernia. It may show a sharp discontinuity of the diaphragm: "gap sign" or "absent diaphragm sign". In patients with suspected PDR, an abnormal air shadow in the cardiac area on chest x-ray study or the presence of air or air-fluid level anterior to the heart on lower chest CT scan is diagnostic (3). MRI has been used successfully to diagnose diaphragmatic injury. However, MRI is not always available in the acute setting and even if it is, many trauma patients require support devices that are not compatible with MRI. Upper GI contrast studies have been used to diagnose TDR. Positive findings include, contrast filled viscera above the diaphragm and obstruction of contrast flow. An echocardiogram may help in differentiating simple PDR from pericardial tamponade (with or without PDR) (7). In our case, the diagnosis was established by Chest x-ray and thorax CT scan and no further investigation was necessitated. PA chest x-ray revealed an elevated left hemidiaphragm and a left decubitus chest x-ray revealed air fluid level in thorax, both were suspicious for a diaphragmatic rupture which was consequently confirmed by thorax CT scan. Although about 90% and 95% of patients with traumatic diaphragmatic rupture also has an associated intra abdominal visceral injury which is another important factor that increases mortality and morbidity, there was no associated intra abdominal visceral injury in our case. The recommended surgical approach in patients with acute and left sided lesions is laparotomy. However, a left sided thoracotomy was performed in our patient because preoperative abdominal CT scan revealed no abdominal pathology. PDR which was diagnosed intraoperatively, was 2 cm in length and wasn't herniated into the pericardial sac. In summary, TDR, and especially PDR can easily be missed in the absence of other indications for prompt surgery. A high index of suspicion combined with repeated and selective radiologic evaluation is necessary for early diagnosis. Therefore, physicians need to be vigilant for these uncommon but important injuries. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}