 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
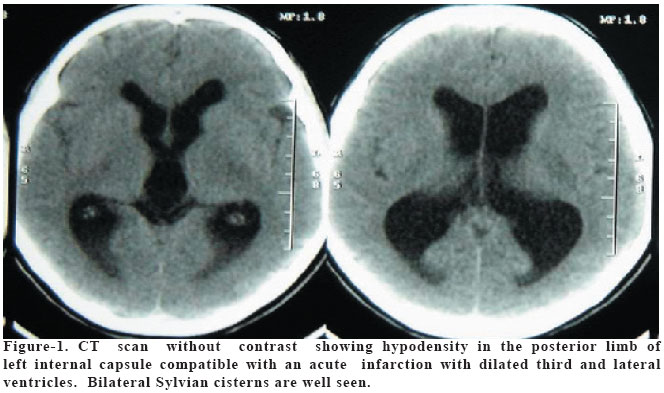
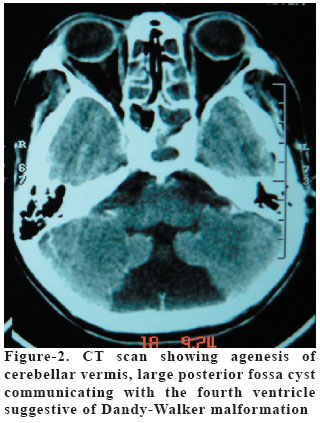
European Journal of General Medicine, Vol. 2, No. 3, 2005, pp. 135-137 HIV INFECTION PRESENTING AS STROKE AND ASYMPTOMATIC DANDY-WALKER MALFORMATION IN AN ADULT Amit Agrawal1, A. N. Hegde2, Lathika Shetty3, Boby Varkey3, J.P. Shetty4 K.S.Hegde Medical Academy, Departments of Neurosurgery1, Internal Medicine2 Radiology3 and Pathology4, Mangalore, India Code Number: gm05029 We report a unique and rare case with definite human immunodeficiency virus infection whose initial presentation was stroke and associated finding of asymptomatic Dandy-Walker malformation in an adult. Key words: HIV, cerebral infarction, stroke, Dandy-Walker malformation INTRODUCTION Human immunodeficiency virus (HIV) infection is a devastating viral infection and neurological dysfunction as the first manifestation of HIV has been found in 10 to 20% of symptomatic patients (1,2). The incidence of clinically evident cerebral infarction in AIDS (Acquired immunodeficiency syndrome) patients varies between 0.5% and 7% (3-5). However stroke as the first presentation of the illness is rare (6). We report a unique case of an adult that presented with stroke as the first sign of AIDS and a rare association of asymptomatic Dandy-Walker malformation. CASE A 40 year female presented with fever of 4 days and sudden onset weakness of right side of body since 2 days. There was no previous history of smoking, systemic arterial hypertension, diabetes mellitus or any significant illness. Her husband was a lorry driver. On examination pallor was present and other general and systemic examination was unremarkable. Neurologically she was conscious, alert and oriented. Motor examination revealed mild weakness of the right side of her face, weakness of grade 3/5 involving right upper and lower limb with hyperreflexia and positive Babinski's sign bilaterally. There were no meningeal signs. Complete blood count revealed Hb-8.6 gm/dl, total white cell count -3,100/mm3 with polymorphs 60%, lymphocytes 38% and eosinophils 2%. Erythrocyte sedimentation rate was 145 mm/Hr. Peripheral blood smear demonstrated microcytic hypochromic red blood cells with an adequate amount of platelets. Blood chemistry and liver function tests were within normal limits. Urinalysis was normal. Antinuclear antibodies, rheumatoid factor, and lupus cell preparation were all normal. Coagulation and protein C were within normal limits. A lumbar puncture was performed, which was unremarkable. Routine Gram stain of CSF and bacteria culture were negative. CSF VDRL was negative. Her serologic tests revealed positive HIV antibody. CT scan of the brain revealed an infarct involving posterior limb of internal capsule (Figure 1). It also showed hypoplasia of cerebellar vermis and large posterior fossa cyst communicating with the enlarged fourth ventricle suggestive of Dandy-Walker malformation and dilated third and lateral ventricles (Figure 2). However sulci and gyri were well seen. She was managed conservatively and started on antiretroviral therapy. She is doing well and hemiplegia improved minimally. DISCUSSION The cause of cerebral infarction or transient neurological deficits in AIDS patients can be found in approximately 50% of cases (7). The most common causes of cerebral infarction in AIDS are nonbacterial thrombotic endocarditis and opportunistic central nervous system infections i.e. toxoplasmosis, cryptococcal meningitis and tuberculosis (2,3,8). However in a good majority of the cases no identifiable cause could be found and the pathogenesis remains unclear (9). It is described that in these patients potential vascular mechanisms for cerebral infarction and transient neurological deficits include a direct toxic effect of viral antigen or vasculopathy caused by HIV (3,10). In our patient no clue was evident indicating impaired immune function up to the onset of hemiparesis. With the available tests, no evidence was present of an inflammation or infection that might be responsible for these ischemic events. No underlying metabolic or cardiovascular disorders were found. Because of the non-reactive VDRL in her CSF, cerebral infarction caused by treponema was unlikely. Therefore we conclude that stroke in this patient was most likely caused by HIV. However, it is not possible to postulate a specific pathogenesis for this ischemic infarction. We presume that ischemic infarction was secondary to vasculopathy caused by HIV. Associated Dandy-Walker malformation in this patient was an incidental finding and she was asymptomatic for that since childhood. Dandy-Walker syndrome is a rare congenital malformation of the hindbrain involving the cerebellum and the fourth ventricle that commonly occurs before the sixth or seventh week of development. It is usually diagnosed at birth or in early childhood. Adult presentation of the Dandy-Walker syndrome is extremely rare (11,12). We could find only one case report where patient never developed evidence of cerebral involvement till adulthood and Dandy-Walker syndrome was an incidental finding (13). This case is unique and rare where the patient presented with ischemic infarct as a first manifestation of HIV infection and also had asymptomatic Dandy-Walker malformation. From the management point of view she is planned to continue on anti-retroviral therapy and close follow-up for Dandy-Walker malformation. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}
{kind=link}