 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
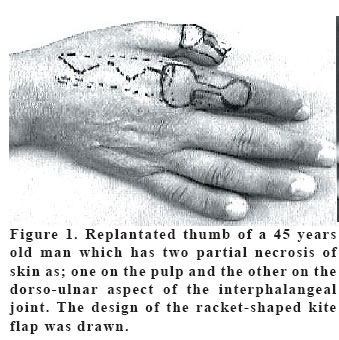
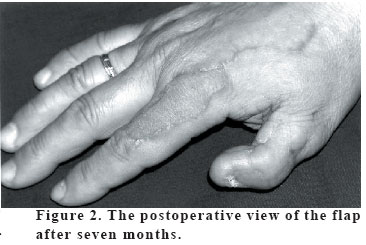
European Journal of General Medicine, Vol. 2, No. 3, 2005, pp. 138-139 LETTER RACKED-SHAPED KITE FLAP Kemal Karaca, Abdullah Etöz, Selçuk Akın Uludağ University, Faculty of Medicine Department of Plastic and Reconstructive Surgery Bursa, Turkey Code Number: gm05030 Traumatic tissue loss of pulp on the first finger, represents a common problem which requires serious reconstructive operations. The final cosmetic appearance and the sensorial sufficiency for an optimum thumb function are important limitations of wound closure during the thumb reconstruction. Generally, these defects are closed by regional flaps as: Palmar advancement flap (Moberg), cross finger flap, neurovascular island flap (Littler) and the first dorsal metacarpal artery flap (Kite) (1,2). In 1964, Moberg described a palmar advancement flap for the pulp reconstruction which was later modified for covering the skin defects of palmar tip of the thumb (3). The thumb defects with bone exposure often require other alternative closure techniques as: Cross-finger flap, Littler flap or Kite flap. The cross-finger flap is a random pattern flap. Attaching the index finger to the thumb for three weeks is obligated. During this period, there are possible handicaps : joint stiffness and contracture of the first web (4). Another alternative is a neurovascular island flap which is raised from the middle finger. During the flap harvest, a very tedious dissection is required to transpose the neurovascular bundle from lateral aspect of the middle finger to the defect of the thumb. Major disadvantage is the donor site morbidity. The first dorsal metacarpal artery flap is another neurovascular island flap which is raised from the dorsum of the proximal phalanx of the index finger. Colema and Holevich described this procedure firstly. But it was popularized by Lie and Posch and modified by Foucher. He incorporated the neural structures into the composite flap tissue and termed it as the Kite flap (5). A 45 years old male who was a machine technician had a saw injury. His right thumb was amputated from the level of proximal phalanx. Immediate tissue replantation was performed. During the first month of the follow-up, two partial necrosis was occurred; one was on the pulp and the other was on the ulnar aspect of the interphalangeal joint in the dorsum of replantated phalanx. After the surgical debridement, bone exposure occured on both defects. We planned a racket-shaped Kite flap for wound closure (Figure 1). A racket shaped Kite flap was planned on the dorsum of the proximal phalanx of second finger. The flap harvest was done under tourniquet. The skin island was racket-shaped but the flap was having a wide rectangular fasciocutanous tissue. The first dorsal metacarpal artery was lying on the fascia of the first interosseous muscle. First dorsal metacarpal artery was identified at the emergence point between the two heads of the first dorsal interosseous muscle. The muscle fascia was cut and the periosteum was stripped from the second metacarp. The subcutaneus veins were dissected carefully and added to the flap pedicle. A subcutaneus tunnel was prepared from the snuffbox to the proximal margin of the defects along the ulnar aspect of the thumb. We released the dense scar tissue and prevented the compression forces to the pedicle. The flap was passed through the incision and sutured to the pulp of the first finger. The donor site on the index finger was covered by using a full thickness skin graft. The patient was followed up for seven months. During this period no wound infection, detachment or loss of skin graft was seen. The final result was satisfactory for cosmetical and functional expectations (Figure 2). In contrast to the two staged procedures, the first dorsal metecarpal artery flap allows immediate postoperative mobilization which outcomes a minimal loss of function and minimal postoperative stiffness (6). The Kite flap may be combined with a radial forearm flap or with a neurovascular island flap in the treatment of the degloving injuries. It should be useful in covering the distal palmar defects of the first finger as an island sensory flap (7). We present a case of two separate defects on the thumb, which were closed succesfully by using a racket-shaped kite flap. To our knowledge, there is no modification about the skin shape of the Kite flap in the literature. It is a new modification of the Kite flap which provides the wound closure of two separate skin defects of thumb by using only one flap. The requirements for thumb reconstruction should force new modifications in using alternative regional flaps. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}
{kind=link}