 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 4, 2005, pp. 144-149 PECULIARITIES OF HEMODYNAMIC CHANGES DURING HIGH THORACIC EPIDURAL ANESTHESIA IN BEATING HEART SURGERY Achurin RS, Lepilin MG, Bajalieva A, Torshin S.V., Lepilin P.M. Russian Cardiology Research Complex, Moscow, Russia Aim: Myocardial protection during off-pump coronary artery
bypass surgery is a multifactorial problem. Careful, individualized choice
of graft sequence and maintenance of stable systemic hemodynamics are of central
importance. Patients with coronary artery disease have a high risk of adverse
cardiac outcome during and after surgery. Thoracic epidural anesthesia (TEA)
aims at a more specific reversible blockade of cardiac sympathetic efferents
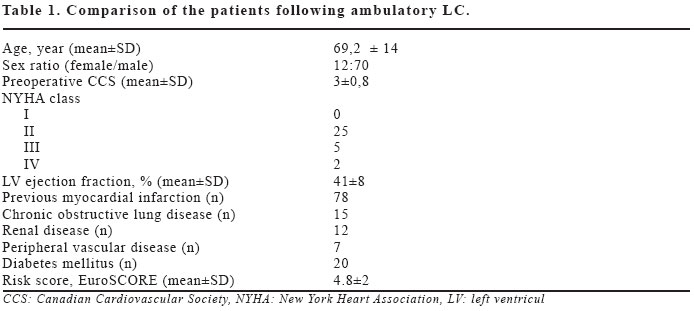
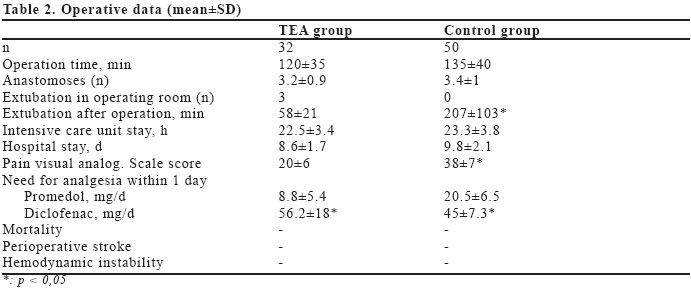
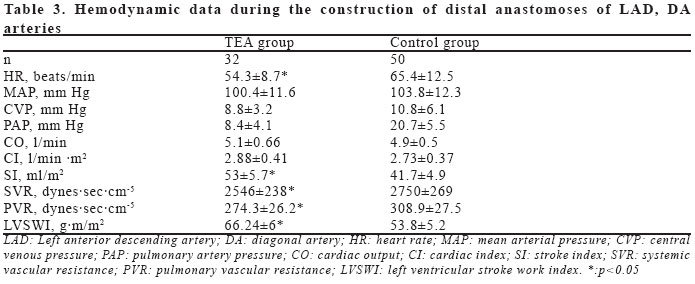
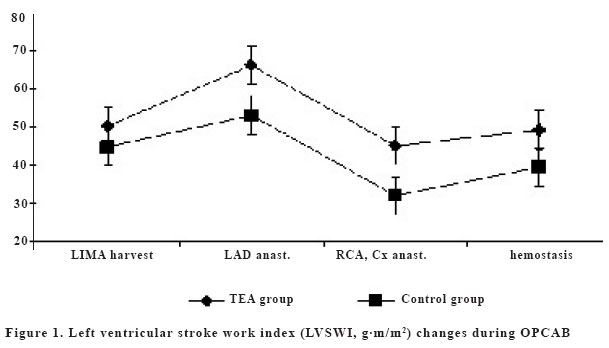
provides effective intra- and postoperative analgesia. Key words: off-pump coronary surgery, high thoracic epidural anesthesia, hemodynamic changes. INTRODUCTION Myocardial protection during operations on beating heart (OPCAB - off-pump coronary artery bypass) is important problem in which the basic questions are individual approach to the choice of sequence of grafts, maintenance of stable hemodynamics and application of various methods for preservation of coronary blood flow (CBF). The short period of ischemia, necessary for construction of grafts and performance of distal anastomoses, may cause a degree of damage in the myocardium not limited to certain zones and may beresulted in myocardial dysfunction at a global level (1,4). The simplest and the most important is the choice of the sequence of the grafts. Widespread tendency to perform left internal mammary artery (LIMA) grafting to the left anterior descending (LAD) first is based on the principle of restoring flow to the left ventricular anterior wall and septum before the vigorous manipulation required to expose the lateral wall of the heart. The right coronary artery (RCА) frequently the dominant one and may create a great risk of ischemia (4). If the degree of stenosis is relatively minor (60-80%), residual flow within the RCA may be high. Thus acute occlusion of the vessel for construction of a distal anastomosis may be poorly tolerated. Bradyarryhythmias may lead to heart failure and profound hemodynamic compromise. Usually this situation is eliminated by epicardial pacer and by use of an intracoronary shunt if a prolonged period of target vessel occlusion is expected for anastomosis construction. Application of intracoronary shunts is limited to their probable damaging action to arterial intima and small diameter of bypassed vessel, however, in case of the dominant right coronary artery, shunt use is justified. The current of blood through the shunt is passive and is much lower than an optimum coronary blood flow, but even the small amount of stream can sometimes provide myocardial perfusion. Well described are temporal intracoronary shunts, in which blood flow is dependant on aortic pressure. Also artificial perfusion systems were developed for perfusion-assisted direct coronary artery bypass (PADCAB), which provide an active current of blood, irrespective of coronary perfusion pressure and arterial pressure (5). Basic anesthetic concept for operations of coronary bypass on beating heart is maintenance of adequate coronary perfusion pressure and reduction of myocardial oxygen demand achieved by heart rate control and moderate decrease in myocardial wall tension. In connection with the requirements to anesthesia high thoracic epidural anesthesia (TEA) is physiologically justified. TEA is directed on more specific blockade of cardiac sympathetic terminations and provides intra and postoperative analgesia. High thoracic anesthesia blocks afferents and efferent fibers, which depart from 5th upper thoracic segments. Painful stimulus is blocked before spinal cord that prevents development of segmental pain caused reactions and stimulation of higher departments of central nervous system. A number of studies (2,6), however now support the use and initiation of further studies of TEA in patients with compromised cardiac function to obtain a definitive answer to this important question. TEA improves cardiac performance and may even have beneficial effects on the oxygen delivery/demand ratio. TEA has beneficial effects on several variables (catecholamines, oxygen balance, coagulation) that correlate with improved patient outcome, although definite proof for better outcome has not been documented. Lung function may also benefit from TEA. Outcome benefit from TEA can be reasonably expected when its intraoperative use is extended to the postoperative period. Questions still remain regarding the application of TEA in anticoagulated patients. Application of TEA in the face of anticoagulation should be undertaken with caution and with consideration of the caveats outlined above. The optimal duration and analgesic regimen of TEA in the postoperative period also remains undefined. Finally, the optimal combination of general anesthesia (inhaled/intravenous) with intraoperative regional anesthesia has yet to be established. Thus, the analysis of modern condition of the problem of myocardial protection has allowed us to conclude that the period of safe coronary artery occlusion is rather individual for each exact patient. Its duration depends on a degree of developed collateral blood flow, initial status of the myocardium, efficiency anesthetic protection and maintenance of hemodynamic stability during the operation. High thoracic epidural anesthesia in combination with general one, now takes the central place for the research, regarding methods of anesthesia for minimally invasive heart operations. The aim of this study was the comparative analysis of clinical efficiency of TEA as a component of inhaled / intravenous anesthesia and traditional anesthesia with opioids during OPCAB. MATERIAL AND METHODS Eighty two patients (12 women, 70 men age 69.2±14 years) with multivessel coronary artery disease underwent OPCAB. Revascularization index was 3.4±1. Patients characteristics are shown in Table 1. To perform total myocardium revascularization during OPCAB in optimal stabilization and positioning of operative field with acceptable hemodynamic values the vacuum myocardial stabilization system "Cosmeya-Tulpan" is used in our department. Operative data are shown in Table 2. All patients were operated with median sternotomy surgical approach. In all cases we used: radial arterial line, continuous cardiac output pulmonary artery catheter, a five lead electrocardiography monitoring with continuous ST segment analysis (Siemens SC 600 2XL , Sweden). Fifty patients (control group 1) were received the traditional balanced inhalation anesthesia (halothane + fentanyl with average dose 3-4mcg/kg/min); 32 patients (TEA group 2) - the combined general anesthesia with TEA using ropivacaine (Naropin, AstraZeneka, Sweden). Anaesthetic management included the use of intravenous fluids, vasopressors (phenylephrine infusion), as necessary to maintain a mean arterial blood pressure of >80 mmHg and cardiac index of >2.1 l/min/m2. An epidural catheter was inserted the night before operation at level Th2 -Th4. All patients received 0.05mg/kg of lorazepam orally as premedication 2 hours before surgery. Anesthesia was induced with propofol 0.8±0.14mg/kg and fentanyl 1.8±0.2mg/kg. Tracheal intubation was performed after deepening of anesthesia with halothane inhalation and muscle relaxation with cisatracurium 0.12±0.02mg/kg. The patients were ventilated with an oxygen/air mixture (FiO2:0.5), and ventilatory settings were adjusted to maintain arterial CO2 tension between 32-42mmHg. After induction of general anesthesia 0.75% ropivacaine was administered epidurally in an average dose of 118±16mg with repeat injection in 3 hours after the first dose as concentration 0.25% concentration. At termination of operation 25mcg epidural fentanyl was administered. After operation all patients were transferred to cardiac surgical intensive care unit. For postoperative analgesia we used continuous epidural infusion of ropivacaine 0.2% with a rate of 3-8ml/hour according to intensity of pain. Statistical Analysis Data are presented as mean ± standard deviation. For comparison of the data a paired Student's test was used. A p value of less than 0,05 was considered to indicate a statistically significant difference. RESULTS Comparison of baseline hemodynamic parameters did not reveal any statistically significant difference between groups. Hemodynamic values obtained during harvesting of left internal mammary artery revealed considerable changes between groups. Heart rate (HR) was 12,6% lower in TEA group, than in control. Despite significant difference between groups in terms of cardiac output (CO) and cardiac index (CI) were lacking, the stroke index (SI) was much higher in TEA group (by 17,4%) suggesting more optimum cardiac function with longer diastole and slower HR, providing maintenance of necessary CI and preventing development of myocardial ischemia. Application of epidural anesthesia promoted reduction of myocardial oxygen consumption due to lower (11,8%) systemic vascular resistance (SVR) in comparison with control group. Pulmonary vascular resistance (PVR) was lower (26,3%) in epidural anesthesia group. The complex of hemodynamic changes developing during high thoracic epidural anesthesia with ropivacaine results in increase in functional heart performance, that is shown by higher left ventricular stroke work index (LVSWI) in comparison with control group (by 12,2%). Hemodynamic changes developing during performance of distal anastomoses to anteriorly located coronary arteries (left anterior descending artery and its diagonal branches), are related to moderate heart dislocation and compression for maintenance of an optimum surgical exposition and a relatively stable operational field (Table 3). Stable hemodynamics and prevention of tachycardia are the important goals for anesthesia which allow to lower risk of myocardial ischemia, occuring with surgical occlusion of coronary artery. Using epidural anesthesia in complex with general anesthesia promoted maintenance of HR by 17% lower than control group, with absence of significant differences in arterial blood pressure. The cardiac index did not differ between groups at this stage, but with lower HR, stroke index was 21.3% higher in TEA group compared to control group (SI, 53.0±5.7 and 41.7±4.9 ml/m2, respectively). When epidural anesthesia was used SVR and PVR were 7.4% and 11.2% lower accordingly: 2546±238 and 274.3±26.2 (dyn·sec/см5m2); than in control group: 2750±269 and 308.9±27.5 (dyn·sec/см5m2). TEA allowed to maintain LVSWI 19.8% higher, than in control group - 66.24±6 and 53.08±5.2 g·m/m2, respectively. DISCUSSION The most expressed hemodynamic changes are observed at a stage of shunting of the coronary arteries located on a back surface of heart-the right coronary, circumflex and posterior descending coronary arteries. The reason of hemodynamic disturbances is significant surgical dislocation of heart caused by application of stabilization system. The basic mechanism is decrease in preload due to mechanical compression of the right heart chambers and as consequence reduced preload of left ventricle, leading to decreased cardiac output and cardiac index. In such circumstances preservation of adequate coronary perfusion pressure can be achieved by increased SVR that prevents or minimizes development of arterial hypotension. The measures to prevent myocardial ischemia at this stage of operation include maintenance of relative bradycardia and normal mean arterial pressure (MAP). Epidural anesthesia allows to keep HR 12.3% lower than control group, and the MAP 5.7% higher, while phenylephrine was infused in both groups. Cardiac output (CO) during epidural anesthesia was by 12,8% (4.36±0.55 and 3.8±0.62 l/min, respectively) higher. Hemodynamic effects of TEA were revealed also at the time of surgical hemostasis, after imposing both distal and proximal vascular anastomoses. In patients receiving epidural anesthesia with ropivacaine: HR was 10.4% lower, CO was 11.2% higher, CI was 11.2%highe, SV was 20.5% higher and LVSWI was 20.0% higher, than control group. Partially changes in TEA group may be explained by better conditions for left ventricular work in the setting of quickly normalized SVR and PVR (by 12.0% and 34.6%, accordingly, than in control group). We suppose that epidural anesthesia allows preservation of left ventricular contractility during and after temporal occlusion of coronary arteries. The most significant differences (p<0.01) between groups were registered in values of SI and LVSWI submitted in Figure 1. Application of high thoracic epidural anesthesia considerably accelerates patients activation and ambulation in the postoperative period. The mechanism of influence of TEA on rate of postoperative activation is reduction of opioids dose, required during and after operation, and achievement of powerful anesthetizing action, not causing postnarcotic depression of consciousness and breath. The general anesthetics are used in combined anesthesia to provide hypnotic and amnesic effects. The dose of fentanyl during operation is reduced by 2,3 times in TEA group. Patients in TEA group waked up in average of 17±15 minutes after operation (84±38 minutes-control group). Patients in TEA group were extubated in 58±21 min., compared to 207±103 min. in control group. Epidural anesthesia provided powerful postoperative analgesia without depression of breath effort. In conclusion, thoracic epidural anesthesia with ropivacaine improves hemodynamic control during operations of coronary revascuralization on beating heart: moderately decreases heart rate, systemic and pulmonary vascular resistance, and provides higher values of cardiac output, cardiac index, stroke index and left ventricular stroke work index, in comparison with sole general anesthesia. Epidural anesthesia, reducing pain during and after operation, is associated with improved physiotherapy cooperation, early extubation, postoperative activation, rehabilitation and reduced risk of depression and posttraumatic stress. The developed method of combined anesthesia with ropivacaine provides adequate anaesthetic myocardial protection during OPCAB, decreases risk of complications and improves results of surgical treatment for coronary artery disease. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}
{kind=link}
{kind=link}
{kind=link}