 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 4, 2005, pp. 153-158 ROINFLAMMATORY CYTOKINES (TNF alpha and IL-6) IN EGYPTIAN SLE PATIENTS WITH
LUPUS NEPHRITIS Alaa A Sabry1, Abdalla M Kalil2, Mona Abd El-Rahim3, Fagr Bazyeed El-Shahat4, Sherief Refat Elbasyouni5 Mansoura University, Departments of Nephrology and Internal Medicine1, Clinical Chemistry2, and Pathology3, Mansoura Urology and Nephrology Center and Medical Biochemistry4, Rheumatology and Rehabilitaion unit 5 , Egypt Aim: Systemic Lupus Erythematosus (SLE) is an autoimmune
disease characterized by a wide variety of autoantibodies, some of which
are pathogenic. In recent years it has become more evident that the polyclonal
B cell activation in SLE is T-cell dependent. To investigate whether serum
levels of TNF-α and IL-6 is higher in Egyptian patients with SLE- presented
with lupus nephritis -than healthy control volunteers and its correlation
with the clinical activity in patients with different activity scores as
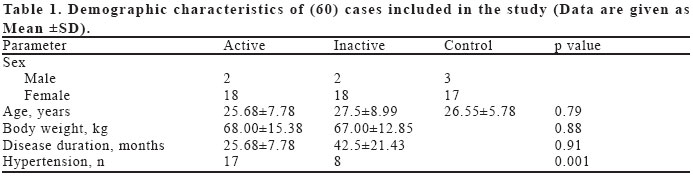
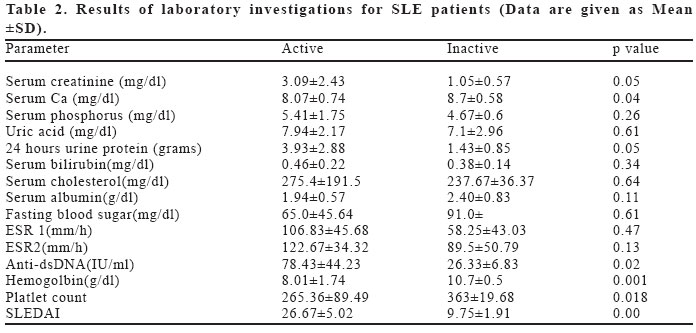
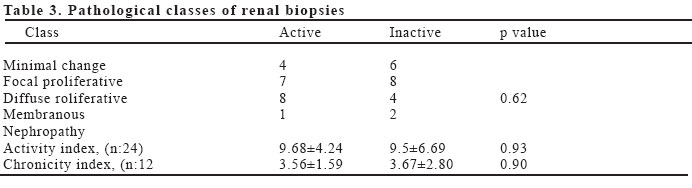
measured by Systemic Lupus Erythmatosus Disease Activity Index (SLEADI). Key words: SLE, lupus nephritis, TNF-α, IL6. INTRODUCTION Systemic lupus Erythematosus (SLE) is a rheumatic autoimmune disease characterized by multisystem organ involvement and by high titers of autoantibodies against several nuclear and cytoplasmic antigens (1). Numerous abnormalities of the cytokine network have been described in patients suffering from SLE as well as in murine lupus models. Some of them were shown to play a pivotal physiopathological role in certain T-cell, B-cell or antigen-presenting cell dysfunctions characteristic of the disease, while others are more likely to be innocent bystanders (2). While many authors concluded that serum TNF α - is clearly elevated and was found to correlate with SLE disease activity (3-5), others reported increased levels only in a minority of patients with active SLE that correlates with thrombocytopenia (6). Meanwhile the role of IL-6 in the pathogenesis of SLE is controversial, While the majority of reports demonstrated increased levels of IL-6 in patients with active SLE that do not correlate with acute phase proteins (7-9), others found elevated IL-6 levels only in cases with increased C- reactive protein , concluding that it is part of the acute phase response (9). Conventional treatment of SLE with immunosuppressive drugs and corticosteroids affects the entire immune system in a nonspecific manner. Although the introduction of these drugs led to markedly improved outcome in SLE there are still patients not sufficiently responding to conventional therapies. The increased knowledge of the pathophysiological mechanisms involved in SLE open the possibility for more specific immunological treatments, targeting, for example, cytokines or cell surface molecules. In view of insufficient data about the role of TNF- α and IL-6 in Egyptian patients with SLE , We conducted this study to assess the levels of TNF- α and IL-6 in sera of 40 patients with SLE presented with lupus nephritis compared with 20 healthy volunteers . MATERIAL AND METHODS Forty patients with SLE and 20 healthy control volunteers served as the subjects of this study. The SLE patients were recruited from the outpatient clinic at Mansoura Urology and Nephrology Center. They presented to the outpatient clinic complaining of symptoms suggestive of lupus nephritis-during the period from January 2003 till February 2004 - and had been diagnosed according to the criteria of the American Rheumatism Association (ARA) (10). All were adults > 18 years, suffering from lupus nephritis (Renal impairment, proteinuria, and or hematuria). Their clinical disease activity was assessed by SLEDAI (11). Twenty SLE patients with active disease (SLEDAI≥10) served as active group (18 female and 2 were male, Mean age 25.68±7.78 year , mean disease duration 25.68±7.78 month and 17 patients were hypertensive), while the remaining 20 consecutive SLE patients with inactive disease -defined as the persistent absence of disease activity (SLEDAI <10) for at least a 4 month period, either without or on a constant dose of immunomodulating drugs (18 female and 2 male, mean age 27.5±8.99 year , average disease duration was 42.5±21.43 month and 8 patients were hypertensive ) were included . Laboratory evaluation Urinalysis, 24 hour urinary protein and venous blood samples were collected for: Serum creatinine, electrolytes, virological analysis (HBsAg, HCV antibodies, CMV antibodies, HIV), changes in levels of anti-dsDNA autoantibodies and Erythrocyte Sedimentation Rate (ESR). Ultrasonic guided renal biopsies were carried out for all patients and examined by one pathologist blinded with the clinical scoring activity of the disease. All biopsies were scored according to histological activity and chronicity index according to WHO classification for lupus nephritis. Twenty healthy volunteers matched for age and sex served as control group where serum samples were obtained for TNF- α and IL-6 assay. All patients gave written informed consent to participate in this study. Measurement of TNF- α and of IL-6 A blood sample was drawn from all participants after an overnight fast and allowed to clot at room temperature for 30 minutes. Sera were separated by centrifugation at 3000 rpm for 15 minutes and separated as soon as possible from the clot of red cells after centrifugation to avoid TNF-α production by blood cells that falsely could increase its values. Separated sera were kept in aliquots at -80 centigrade until the time of assay. Sera were assayed for TNF-α using ELISA kit according to Aderka et al 1992 (12) and for IL-6 using ELISA kit according to Brailly et al (13). Statistical analysis All data were expressed as frequencies or mean and standard deviation. Comparison of quantitative data was done using T-test. Chi-square test was used for comparison of qualitative data. P value less than 0.05 was considered as statistically significant. Pearson correlation test was used to analyze the correlations between various laboratory measures and the SLEDAI score. SPSS package 9.05 for windows was used. RESULTS SLE patients and healthy control volunteers were matched regarding age and sex. No statistically significant difference were observed between those with active and inactive disease regarding age, sex, body weight, and disease duration. Seventeen patients in the active group were hypertensive compared to only 8 patients in the inactive group, this difference was statistically significant (p=0.001). The demographic characteristics of the active and inactive SLE groups are given in Table 1. While serum creatinine, 24 hour urine protein, anti-dsDNA were all statistically significantly higher, hemoglobin and platelet counts and calcium level were statistically significantly lower in the active group compared to the inactive group. Phosphorus level, uric acid level, prothrombin concentration, serum bilirubin, ESR - first and second hour-, Serum cholesterol, albumin level, fasting blood sugar were comparable in both groups (Results of laboratory investigations are given in Table 2. Serum TNF alpha The mean level of serum TNF- α was significantly higher in SLE patients with active disease when compared with those with inactive disease (766.95±357.82 ρg/ml versus 314.01±100.87 ρg/ml (p=0.002). It was also significantly higher in SLE patients with inactive disease compared with the healthy control group (314.01±100.87 ρg/ml versus 172.7±39.19 ρg/ml, p=0.000). Serum IL-6 level The mean level of IL-6 was statistically significantly higher in SLE patients with active disease when compared with those with inactive disease (135.4±54.23 ρg/ml versus 47.33±18.61 ρg/ml, p=0.002) .At the mean time it was significantly higher in SLE patients with inactive disease compared with the healthy control group (47.33±18.61 ρg/ml versus 21.15±10.99 ρg/ml , p=0.000). Correlation between TNF- α and IL-6 and SLEDAI There was a positive correlation between serum TNF- α , IL-6 and SLEDAI (r = 0.743 and 0.772 respectively. Renal biopsy findings There were no statistically significant differences regarding the class, activity and chronicity indices of the renal biopsy findings between both groups. The pathological classes of the renal biopsies are described in Table 3. DISCUSSION Systemic lupus erythematosus is a prototypical autoimmune disease characterized by a variety of autoantibodies (14). The pathologic events in SLE are mediated by the formation of immune complexes, activation of the complement cascade. These autoantibodies and the consecutive formation of immune complexes apparently constitute the major pathophysiological force of lupus disease, ultimately inflicting injury on a variety of organ systems (15). The ensuing inflammatory process may then lead to progressive tissue destruction and organ damage, such as lupus nephritis, a common and serious manifestation of SLE. The role of proinflammatory cytokines in the pathogenesis of SLE as well as the effect of cytokine blockade is still controversial. Several studies have investigated the cytokine profile of SLE patients in vivo and in vitro. Despite the inconsistent findings of either increased or decreased levels of interleukins (IL-2, IL-4, IL-6, IL-10) or TNF-α in SLE patients in comparison with healthy controls, these studies confirm that SLE patients display an altered cytokine profile (16). TNF- α is both a proinflammatory and an immunoregulatory cytokine with differential effects on B cells, on T cells and on dendritic cells as well as on the process of programmed cell death which could explain its role in SLE. TNF-α is a growth factor for B lymphocytes, and B lymphocytes are able to produce significant amounts of TNF- α in an autocrine loop (17). It is of interest that this autocrine TNF- α production is induced by ligation of CD40, a possible therapeutic target in SLE, and is prevented by cyclosporin A, another therapeutic agent for SLE (18). TNF- α was reported to be highly expressed in glomeruli in all forms of lupus nephritis, and the degree of TNF-α expression correlates with renal inflammatory activity (3) as measured by a histological activity index. This correlation again suggests involvement of TNF-α in the inflammatory and destructive process of the disease (19). Several studies have investigated the level of TNF-α in patient with SLE, to our knowledge only one study (20) focused on TNF-α and soluble tumor necrosis factor receptor II (TNFR II) in Egyptian patients with SLE that included few patients with lupus nephritis and did not address IL-6 as a marker of disease activity. In the present study serum level of TNF- α and its correlation to disease activity in 40 Egyptian patients with SLE presented with lupus nephritis with different scores of activity were investigated. The level of TNF-α was significantly higher in SLE patients when compared with the healthy control volunteers; furthermore it was also statistically significantly higher in SLE group with active lupus when compared with SLE patients with inactive disease. Despite the fact that these data are in agreement with most of what reported in the literature (3-5,20), it is not in full agreement with the only report from Egypt (20) which found a correlation between TNF-α levels in his group of SLE patients and SLEDAI but further concluded that the level of TNFR II to be the only predictor of SLE disease activity among Egyptian patients . We did not investigate for TNFR II in our patients as a direct relation between TNF-α serum level and TNFR II was previously reported (21). The difference in patients clinical presentation- in this study (20) 30 patients presented with neuropsychiatric lupus erythematosus, 28 with vasculitis while in ours none had these manifestations may in fact be responsible for the this controversy. In another study (6), serum levels of TNF -α were found to be elevated in most patients with SLE associated with thrombocytopenia and within the normal range from patients with SLE associated with nephritic syndrome, lupus nephritis, or central nervous system disease, this controversy could be explained by the fact that SLE is a genetic disease (22) and we can assume that the difference in the genetics of different populations may be responsible for the difference in clinical presentation. IL-6 which is the second target in our study-is a pleiotropic cytokine with a wide range of biological activities that plays an important role in immune regulation and inflammation. An association between IL-6 and lupus was demonstrated in murine models of SLE and blocking IL-6 improved lupus in all models tested (23). IL-6 is one of the most important B cell stimulating factors that induces the differentiation of T cells into effector cells. Its reduction could explain findings from clinical trials and animals studies that anti-CD4 therapy decreases autoantibody production in vivo (24). IL-6 is highly expressed in kidneys in human lupus glomerulonephritis (25), IL-6 promotes disease in NZB/W mice; treatment with anti-IL-6 antibodies may delay nephritis (26) indicating that blocking IL-6 may be another valid therapeutic approach. The role of IL-6 in the pathogenesis of SLE is also controversial. While some authors found elevated IL-6 levels only in cases with increased C-reactive protein, concluding that it is part of the acute phase response (7) , others reported high levels in the cerebrospinal fluid in cases with CNS involvement (27). Results of our study are in agreement with most of these reports since IL-6 level is significantly increased in Egyptian patients with SLE and lupus nephritis (Mean 93.68±60.46) when compared to healthy control patients (21.15±8.89, p: 0.00). IL-6 was also significantly higher in SLE patients with higher SLEDAI score being (135.4±54.23) in those with active disease compared to (47.33±18.61) in SLE group with inactive lupus (p: 0.002). Our data indicate that IL-6 is elevated in SLE patients with lupus nephritis whether they have active or inactive disease even without CNS involvement. The biochemical marker of renal involvement (Serum creatinine, 24 hour urinary protein, level of Anti-dsDNA) were all higher in the active group, however the striking feature is the absence of significant diference in the activity or chronicity scores in renal biopsy obtained from the active and inactive SLE groups . However a lack of correlation between serum creatinine and pathological data was previously reported (28) and in such cases it is better to consider creatinine clearance rather than serum creatinine as a laboratory indicator of renal function. Thus, our data allow us to speculate that, Egyptian SLE patients with lupus nephritis have altered cytokine profile different from their healthy control subject. TNF- α and IL-6 are significantly increased in Egyptian SLE patients with Lupus nephritis compared to the healty control subject and this level is well correlated with SLE disease activity. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}
{kind=link}
{kind=link}