 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 4, 2005, pp. 164-166 INTRADURAL DISC HERNIATION A case report and review of the literature Nebi Yılmaz1, Nejmi Kıymaz1, Ömer Etlik2, Çiğdem Mumcu1 Yüzüncü Yıl University, Faculty of Medicine, Departments
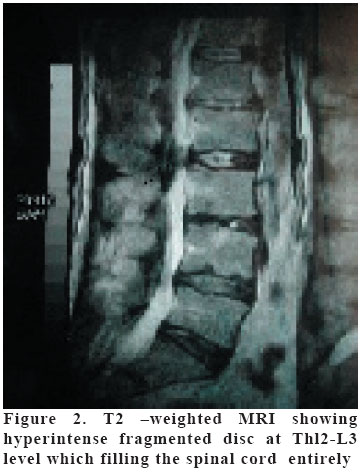
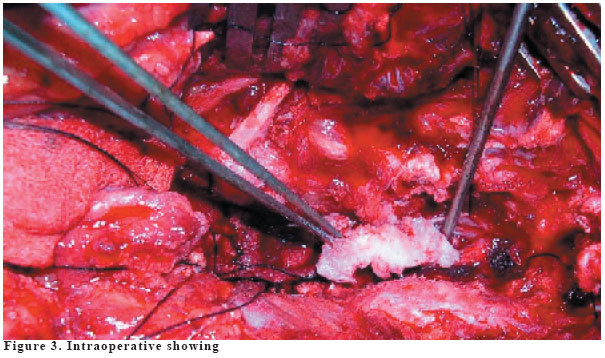
of Neurosurgery1 and Radiology2, Van, Turkey. Code Number: gm05036 Intradural disc herniation (IDH) is a rare pathology. Intradural disc herniations comprise 0.26-0.30% of all herniated discs. The preoperative knowledge of an intradural herniation is important because it has an influence on the operative strategy. A 55-year-old man suffered from decrease in the motor function of the lower extremities and urinary incontinence. Noncontrast MRI exam showed the intradural disc with caudal migration of an excluded fragment at the L3-4 level. At surgery, the L3 and L4 laminas were removed and after dura had been openned, a nucleus pulposus was seen which compressed the conus medullaris to the right and left of the spinal canal. Every neurosurgeuon involved in spinal surgery must be aware of this rare patology which, when overseen during the intervention, could have disastrous consequences for the patient. Key words: Intradural disc, surgery, cauda equina syndrome INTRODUCTION Intradural disc herniation (IDH) is a rare pathology. Intradural disc herniations comprise 0.26-0.30% of all herniated discs. In all, 5% are found in the thoracic, 3% in the cervical, and 92% in the lumbar region (1,2). The first report of an intradural herniation was presented by Dandy in1942 (2). The preooperative diagnosis of IDH is still difficult, despite new neuroradiologic investigation possibilities including computerized tomography (CT) and magnetic resonance imaging (MRI). CASE A 55-year-old man suffered from decrease in the motor function of the lower extremities and urinary incontinence. At admission, neurological examination revealed; decrease in the motor function of the lower extremities in one-fifths, loss of patella and achilles tendon reflexes, and bladder dysfunction. Hypoesthesia of the left and right S1, L5 and L4 dermatomes were found. He had no back pain and Lasègue's sing at 90º. Noncontrast MRI exam showed the intradural disc with caudal migration of an excluded fragment at the L3-4 level. At surgery, the L3 and L4 laminas were removed and after dura had been openned, a nucleus pulposus was seen which compressed the conus medullaris to the right and left of the spinal canal. This disc material was removed with ceruful microdissection. The disc fregment had pierced the ventral wall of the dura. The operation was ended after primary closure of the defect with fibrin glue. The postoperative course was uneventful and when seen again 4 months later, the patient was able to walk. DISCUSSION Migration of the disc nucleus pulposus in the intradural site requires perforation of the annulus fibrosus of the posterior longtudinal ligament and the dura mater (3). The physiologic and patological feature that cause this event are unclear, even though several reasons are known that may contribute to the formation of intradural herniation. 1. Congenital narrowing of the spinal canal with less epidural space, 2. Adhesions between the annnulus fibrosus, posterior longitudinal ligament, and duramater, 3. Congenital and iatrogenic fineness of the dura mater (1,4,5). In our case , the adhesions were prominent. Preexisting degenerative spondilotic changes and the chronic herniated disc may have contributed to adhesions. Perhaps the most likely cause was mechanical irritation due to the chronic disc herniation against the ventral wall of the dura. The treatment of intradural disc herniations basically involves surgical removal of ruptured disc meterial. At surgery, the dura and root must be carefully explored. Closure of the ventrally located dural tear is necessary because of the risk of CSF leakage. Intradural disc need to be recognized and treated appropriately at the time of the initial operation to prevent the development of the back failure (6,7). Cauda equina syndrome and sphincter disease have an incidence of 30% of all reported cases, as in our cases (1). Howewer, there may be cases where the disc protrudes intradurally to compress a single root and show single only of root compression. Intradural disc herniation above the conus medullaris seems to bring on neurologic dysfunctions more rapidly (6). In the myelographic examination, intradural disc herniations of the lumbar region usually show as a complete block (8). Although CT and postmyelogram CT can provide valuable information regarding intradural lumbar disc herniation with MRI as reported by Epstein (2) and Jenkine (3). It is usually not difficult with current MRI techniques to differentiate lumbar disc herniation from other conditions. The MRI finding of an intradural lesion raises several diagnostic doubts that must be considered and resolved with differential diagnosis, which includes neurinoma, meningioma, ependymoma, and dermoid. Neurinoma end meningioma both have homogeneous enhancement and clearly different from the ring enhancement of intradural herniations. The site most frequently affected is L4-5 (55%), followed by L3-4 (16%) and L5-S1 (10%) (5,9). Even more rarely, ruptured disc fragment may migrate intrathecally. According to the commonly admitted theory, this migration may be facilitated by the existence of adhesions between the posterior longitudinal ligament and the anterior ligament (3,10). As a result, during the disc operation, every neurosurgeuon involved in spinal surgery must be aware of this rare patology which, when overseen during the intervention, could have disastrous consequences for the patient. REFERENCES
Copyright 2005 - Medical Investigations Society The following images related to this document are available:Photo images[gm05036f2.jpg] [gm05036f3.jpg] [gm05036f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}