 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
European Journal of General Medicine, Vol. 2, No. 4, 2005, pp. 173-176 ANTIPHOSPHOLIPID SYNDROME PRESENTING AS MASSIVE PULMONARY EMBOLISM IN A PATIENT WITH SARCOIDOSIS Bahar Artım Esen1, Esen Kıyan2, Reyhan Diz Küçükkaya3, Levent Tabak2, Faruk Aktürk1, Orhan Arseven2, Gülfer Okumuş2, Murat İnanç4 İstanbul University, İstanbul Faculty of Medicine, Departments of
Internal Medicine1 and Respiratory Medicine2,
Division of Hematology3 and Rheumatology4, İstanbul,
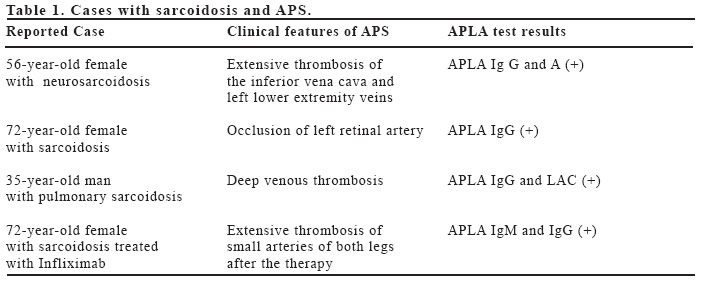
Turkey Code Number: gm05039 Antiphospholipid antibodies may be detected in sarcoidosis generally without clinical consequences. The association between sarcoidosis and antiphospholipid syndrome was rarely reported. Herein a case with sarcoidosis and antiphospholipid syndrome presenting as massive pulmonary embolism is presented. Key Words: Sarcoidosis, thrombosis, antiphospholipid syndrome INTRODUCTION Sarcoidosis is a systemic, chronic disease of unknown etiology that is characterized by non-caseating granulomas in any tissue. Impairment of cellular immunity is known to play a major role in this disease. Humoral abnormalities such as the occasional presence of anti double-stranded DNA (anti- ds DNA), antinuclear antibody (ANA) and rheumatoid factor (RF) have also been observed in patients with sarcoidosis but the clinical significance of these autoantibodies is not known (1-3). Although the presence of antiphospholipid antibodies (APLA) have been reported, the occurrence of antiphospholipid syndrome (APS) seems rare. Herein, we report a case of massive pulmonary embolism due to APS with additional thrombotic risk factors who also had multiple mediastinal and hilar adenopathies that were diagnosed as sarcoidosis. CASE A 29 -year-old female was admitted to the emergency department with shortness of breath, chest pain, nausea, and vomiting. She was obese with a history of hypertension and hyperlipidemia. She noted oligomenorrhea for which she had been prescribed an oral contraceptive drug containing 2 mg of cyproterone acetate and 0.035 mg of ethinylestradiol six months ago. She did not smoke and there was no personal or family history of thrombosis or miscarriages. On examination she was in severe respiratory distress. An arterial blood sample at room air revealed a PO2 of 68 mmHg, a PCO2 of 20 mmHg. An electrocardiogram showed sinus tachycardia at a rate of 120, with an R-wave axis, 2 mm of ST segment elevation in leads V1 through V3; T waves were inverted in leads III and V2 through V4. Blood biochemical evaluation disclosed a serum LDH of 505 U/L (normal 240-480 U/L), AST 62 U/L (5-42), ALT 93 U/L (5-45) and GGT 98 U/L (5-85). There was neutrophilic leucocytosis on her leucocyte differential; platelet count and hemoglobin values were within normal limits. APTT was 42 sec (24-32) while PT was within the normal range. Echocardiography demonstrated dilatation of the right ventricle, severe pulmonary hypertension with a pressure of 70 mmHg, enlargement of the pulmonary artery and 2-3 (+) tricuspid valve insufficiency. The perfusion scan indicated high probability pulmonary embolus. The spiral computed scan of the thorax showed a thrombus in the right main pulmonary artery as well as in the segmental branches of the left pulmonary artery. No abnormalities of the lung parenchyma were detected. CT scan also revealed lymphadenopathies at both hilar regions and at stations 2R, 4R, and 7, with the largest nodes measuring 1.5 cm in diameter. The patient was anticoagulated with intravenous heparin, and then was maintained on warfarin. In the meantime, the procoagulant risk factors other than her obesity and use of oral contraceptive drugs were investigated. Laboratory studies showed that levels of Antithrombin III, Protein S and Protein C were within normal limits. Factor V Leiden and prothrombin G20210A mutations were absent. The anticardiolipin antibodies (ACLA) IgG and IgM were negative. On the other hand, lupus anticoagulant (LAC) was found to be positive by coagulometric assays. Transbronchial lung biopsy and fine needle aspiration biopsy of mediastinal lymph nodes that appeared at her CT scan were performed. The histopathological examination disclosed noncaseating granulomas. Lower lip minor salivary gland biopsy revealed a granulomatous sialadenitis which was consistent with sarcoidosis. A whole body scan with gallium - 67 showed multifocal increased activity at the hilar and parahilar regions which supported sarcoidosis. On 20th day of admission, a control thorax CT scan and echocardiography were performed. The area of thrombus was smaller, right heart size became normal and pulmonary pressure was 40 mmHg. Seven weeks after the initial evaluation, lupus anticoagulant and anticardiolipin antibodies were studied for the second time. Lupus anticoagulant was found positive again, ACLA Ig M was 22 MPL ( 0- 10), and ACLA Ig G 20 GPL. The patient was diagnosed as APS and she fulfilled the preliminary classification criteria of APS (4). After 8 months of anticoagulation, the CT scan revealed no signs of thrombus but infiltration of the lung parenchyma with sarcoid granulomas. During the patient's follow-up LAC remained persistently positive. The ACLA were positive on her last visit with titers being 30.5 and 24 U/ml for IgM and IgG respectively. DISCUSSION APS is a disorder characterized by thrombosis and/or pregnancy loss associated with antiphospholipid antibodies. It is mostly associated with systemic lupus erythematosus but coexistence with other connective tissue diseases has also been reported. Documentation of the presence of antiphospholipid antibodies can be either by a solid phase assay (anticardiolipin) or by a test for an inhibitor of phospholipid-dependent clotting (lupus anticoagulant) (5). Suggested pathophysiological mechanisms that cause a hypercoaguble state in APS include disruption of the kinetics of the normal procoagulant and anticoagulant reactions occurring on cell membranes and alteration of the expression and secretion of various molecules because of stimulation of certain cells by APLA (6). Pulmonary thromboembolic disease which may be the first manifestation of the disease, constitutes the most common pulmonary manifestation of the APS. Besides pulmonary embolism, other pulmonary manifestations of APS include pulmonary hypertension, adult respiratory distress syndrome (ARDS), intra-alveolar haemorrhage and primary thrombosis of lung vessels (7). Sarcoidosis is a chronic multisystem granulomatous disorder with impairment of cellular immunity. There is an inflammatory response characterized by activated macrophages and CD4 helper lymphocytes. It is thought that persistent antigens trigger the helper-inducer T cells and exposure of genetically susceptiple hosts to these antigens results in sarcoidosis (8). Humoral immunological abnormalities such as increased levels of immunoglobulins and autoantibodies including ANA (29%), RF (20-40%) and anti-ds DNA (6%) have been reported in patients with sarcoidosis (1,3,9). The clinical significance of these antibodies is not known but their existence has been considered to be suggestive of a shared immunopathogenic mechanism with connective tissue disorders. Sarcoidosis has also been reported to coexist with various autoimmune diseases such as rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), systemic sclerosis (SSc), and Sjögren's syndrome. In a review of 569 patients with different autoimmune diseases like RA, primary Sjögren Syndrome and SLE, the incidence of sarcoidosis was found to be 1% (2). Another study with 300 SLE patients reported the incidence of sarcoidosis in SLE patients as 1% (10). Previously the presence of APLA was reported in patients with sarcoidosis but the associated clinical syndrome was found to be rare. A Japanese study published in 1994 , investigated APLA in 55 patients with sarcoidosis and 38% of the patients were found to be positive for either IgG or IgM APLA which was significantly higher than that of healthy controls (11). In this study, these antibodies were not associated with APS in these patients but there was a significant correlation with the presence of extrapulmonary disease. Reported cases with sarcoidosis and APS are summarized in Table 1 (12,13,14,15). Thrombotic events within the course of sarcoidosis have also been observed but APLA were not measured in all cases. The patient we report here presented with a massive pulmonary emboli. The etiology of thrombosis in our patient seems to be multifactorial. Obesity, oral contraceptive usage, hyperlipidemia, hypertension along with the existence of LAC were the factors that might have led to a massive thrombotic event. It was suggested that oral contraceptives may trigger the formation of thrombosis in patients with LAC and/or ACA (16,17). In this patient the search for procoagulant factors confirmed the persistent presence of lupus anticoagulant which fulfill the diagnostic and classification criteria of antiphospholipid syndrome (4). Life-time anticoagulation in this patient seems warranted since she had experienced a life-threatening thrombosis and persistent presence of LAC had been confirmed. She was not at an advanced stage of sarcoidosis and did not have any extrathorasic manifestations of the disease. The mechanical effect of the sarcoid granulomas may cause thrombosis in patients with sarcoidosis, but it is not clear whether sarcoidosis by itself carry a procoagulant potential or formation of thrombosis is triggered by the existence of additional risk factors (18). In conclusion, both APLA and APS may occur in patients with sarcoidosis. In patients with sarcoidosis APLA must be investigated when appropriate clinical features (e.g. fetal loss, thrombosis) are present. Immune abnormalities including the presence of APLA are reported in sarcoidosis but the association with APS which is an autoimmune disease has been rarely reported. Although unrelated immunologic abnormalities were detected in patients with sarcoidosis and APS, it is not known whether a common stimuli trigger both diseases. REFERENCES
Copyright 2005 - Medical Investigations Society |

{kind=link}