 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
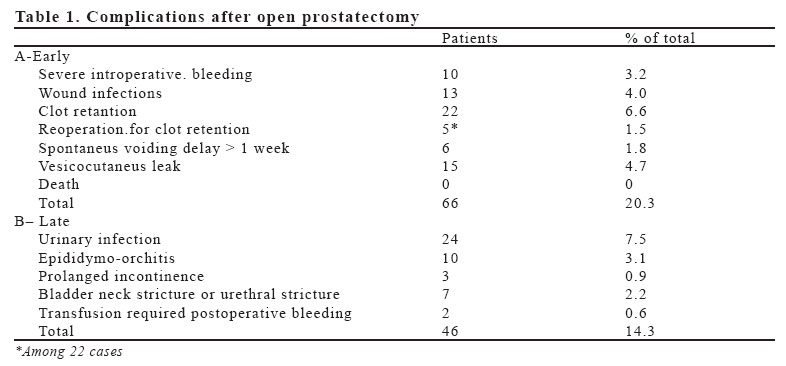
European Journal of General Medicine, Vol. 3, No. 1, 2006, pp. 11-15 OPEN PROSTATECTOMY - THE RESULTS OF A SERIES OF 320 CASES IN RURAL AREA Kadir Ceylan Yuzuncu Yıl University, Faculty of Medicine, Department of Urology Van, Turkey Correspondence: Kadir Ceylan, MD Yüzüncü Yıl Üniversitesi Tıp Fakültesi Üroloji A.D. Van –Türkiye Tel: 905335130407, Fax: 904322156195 E-mail: akceylan2000@hotmail.com Code Number: gm06003 Aim: Suprapubic prostatectomy is frequently performed in areas with poor socioeconomic condition due to insuficient endoscopy equipment. The aim of this retrospective study is to analyse and bring our experience about the open prostatectomy operation Key words: Open prostatectomy, rural area, complication INTRODUCTION Benign prostatic hyperplasia (BPH) is the most common benign tumor in men and its incidence is age-related (1). The estimated prevalence is 25 % in men aged 40 to 79 years.(2) The treatment of urinary bladder outlet obstruction secondary to BPH is pharmacologic (medical) and surgical. Prostatectomy for patients with BPH is one of the most frequent operations performed in the world (3). Until 20-25 years ago, while open surgery was the most common approach, in the late 1970s, the development of endoscopes gradually reduced open surgical operations (3). However, current indications mainly consist of large adenoma, especially in which there is a coexistent pathology that can be easily managed transvesically, such as large bladder diverticulum or bladder stones (4). The ratio of open surgery to endoscopic resection has larger variations among different countries. Endoscopic resection needs endoscopic equipment and expertise. Suprapubic prostatectomy may be safely performed in areas with poor socioeconomic condition by adequately trained surgeons who have no sufficient endoscopic equipment. In rural areas of many countries and in some rural areas of our country, patients do not usually admit for treatment until they have acute urinary retention, even though they have had diminishing caliber and strength of the urinary stream for months. The aim of this retrospective study is to analyze and bring our experience about the series of 320 patients underwent open prostatectomy operation, the open method which is preferred by both doctors and patients due to various reasons especially in rural areas and most of the public hospitals in our country, in terms of bladder catheter staying time and postoperative bleeding control. MATERIALS AND METHODS We report a retrospective study of 320 consecutive patients who presented with lower urinary tract obstructive symptoms and an enlarged prostate gland on digital rectal examination and suprapubic ultrasonograpy (US). All patients underwent suprapubic transvesical prostatectomy in Osmaniye Public Hospital between October 1996 and December 2002. Indications for open prostatectomy included large prostate glands, which was greater than 50 ml by suprapubic US. Subsequent suprapubic US was used to measure the post-voiding residual urine volume. Patients with smaller prostate volumes were also included in the study because of associated conditions, such as inguinal hernia, large bladder diverticula or bladder stones. Analyzed factors were; age, complaints, co morbidities, (especially cardiac and respiratory), early and late complications and mortality. Patients with co morbidities were treated prior to operation. Surgical technique Open prostatectomy was performed under general or regional anesthesia after obtaining informed consent. Suprapubic Pfannenstiel incision was made in all patients. A longitudinal incision was used to enter the bladder, and bladder cavity was controlled before the enucleation. The urethral orifices were identified and protected from injury during the procedure. A circumferential incision was made around the urethral orifice at the bladder neck, followed by digital enucleation of the adenoma. After removal of the adenoma, additional wedge resection to bladder neck was performed to facilitate urethral catheterization and the places of visible bleeding at the incised edge of the bladder neck were controlled with electrocoutery and a continue haemostatic suture was placed between 3 to 9 o’clock (chromic cat-gut 2/0). A 20-22 F three-way irrigating Foley catheter was passed through the urethra , the balloon was inflated to 50-60 ml and the balloon was left in the bladder. The traction procedure was applied to the catheter to compress the bladder neck in patients with bleeding risk. The bladder was closed in three layers with a running absorbable sutures (chromic 2/0). Extravesical drain was used. Abdominal wall and skin was closed . Continuous saline irrigation was administered until the clearance of clot and gross bleeding. Traction procedure lasted usually for six to twelve hours. In most cases, urethral catheter was removed at the second day, and patients were discharged at the fourth day postoperatively. Histopathological evaluations of prostate specimens were done in all patients routinely. Patients were controlled at the seventh day for wound examination. For antibiotherapy quinolones were administered intravenously as 200 mg /iv single dose preoperatively and at 12th and 36th, quinolone treatment was continued orally for 21 days. RESULTS The mean age of 320 patients was 73 (range 52 to 100 years). Many patients were elderly men who presented to an emergency clinic with acute urinary retention and underwent emergent bladder decompression, usually with a urethral catheter (142 patients). Suprapubic cystostomy using cystofix was rarely needed. Others were patients with urinary obstruction symptoms manifested by frequency, urge incontinence, nocturia greater than 3 times, hesitancy and depressed projection and calibration of urine. Eighteen patients had undergone transurethral resection of the prostate previously. Prostatic enlargement had developed again in these patients. Fifty-two patients with BPH had also one or multiple bladder stones and/or giant diverticules (determined with US preoperatively). Thirty-two patients underwent simultaneous inguinal herniorraphy. In 220 cases with clear urine, catheters were removed at the second day, while in the remaining 100 cases with hemorrhage, catheters were removed at the third day. In no case catheter usage was needed more than 3 days. Prostate specimens of 18 patients showed prostatic carcinoma. Two hundered and thirty of the 320 patients (72%) had comorbidity. Early complications were cardiovascular and respiratory morbidities, urine leakage, wound infection, and hemorrhage. Cardiovascular or respiratory problems developed in 68 patients and these patients were treated (with internal medicine consultations) and all patients did well. Clot retention developed in 22 patients within 24 hours. After the operation, seventeen of these responded to intermittent syringe irrigation but 5 required evacuation or cystotomy by endoscopes sheath. Two patients had clot retention within two weeks after discharge, and, evacuation was insufficient as a therapeutic procedure. These patients needed endoscopical coagulation as well. All of these patients and patients with intraoperative severe bleeding received blood transfusions (totally 32 patients). Wound infections were treated topically and systemically. Six patients were unable to void properly after removal of the urethral catheter, and urethral catheter was inserted and remained for additional one week, after reremoval of the second catheter time they were able to void satisfactorily. Urine fistula through the wound was developed in 15 patients These patients were treated with urethral catheter placement and these fistulas were closed spontaneously within the subsequent 2 or 3 weeks, then catheters were removed. Late complications included: bladder neck and urethral stricture (n:7), prolonged incontinence (n:3), bleeding requiring blood transfusion (n:2), epididimo-orchitis and urinary infections (n:10, n:24 respectively). Patients with bladder neck stricture and urethral strictures were treated by dilation or visual internal urethrotomy. Complications of open prostatectomy were summarized in Table 1. DISCUSSION For surgical management of BPH, open prostatectomy is the most efficient therapeutic option for the relief of symptoms and urine flow improvement, but it is also more invasive and morbid compared to other surgical procedures.Transurethral resection of the prostate (TUR-P) is still the gold standard for treatment of BPH. TUR-P is as efficient as open prostatectomy, less invasive, less expensive and with less morbidity, thus it has become the gold standard for the treatment of BPH (5). But open prostatectomy has been reported to have lower per operative mortality than TUR-P and low retreatment needs and thus reduce the long-term cost. TUR-P is available only in major centers with trained specialists and resectoscopic equipment (6). Because of these reasons, I have chosen the open prostatectomy as surgical procedure, and also I especially recommend open prostaectomy to patients with large prostate volumes (> 50 ml). McGill and Belfield described Suprapubic transvesical partial enucleation of the prostate in the late 1800s. However it was until Fuller and Frayer (7) that the complete enucleation of the gland gained widespread acceptance. Mortality rates in the early years were about 10%, owing primarily to pre-existing uremia, debilitation and postoperative hemorrhage. By time operative mortality rate decreased (6), but postoperative hemorrhage remained as a serious problem. The concept of control of postoperative hemorrhage by separation of the bladder neck from the prostate fossa was presented by Lower and Harris (7) Using non-absorbable bladder neck suture, Hryntschak modified and popularized this technique in 1951. Dela Pena and Alcina proposed separation of the bladder cavity from the prostate fossa using a removable purse-string suture in 1962 (7). Malement popularized the removable partition suture, which is recommended only in cases of excessive bleeding in textbooks (8-9). In our study, visible bleeding after adenoma removal at the incised edge of the bladder neck was controlled with electrocoutery and haemostatic sutures. Additionally, Foley catheter balloon was inflated to 50-60ml, and the catheter was left in the bladder in all patients. The traction was applied to the catheter in order to compress the bladder neck by attaching the catheter on one leg with sticking plaster for 6 to 14 hours. Clot retention was occurred in 22 cases. A probable causative factor for hemorrhage was considered as the loss of traction force due to inadequate nursing care. When the literature rewieved, an advocation of continuous bladder irrigation via the three-way Foley catheter for 12 to 24 hours was found. The Foley catheter is usually removed after 3 days, and the suprapubic catheter is clamped at 5 days to give the patient a trial at voiding. The drain is usually removed a few hours following removal of the suprapubic tube if there was no drainage.( 9-10-11 ). Contrary to the common intervention, we removed the catheters after 48 hours when the urine was clear and we didn’t use any suprapubic catheter .The drain was removed one day following removal of the urethral catheter if there was no drainage. When this approach was compared to traditional one such as Condie’ s study there was no difference in terms of complications but only urine leakage (1% us 4.7% respectively). This complication was seen only in patients with previous urinary retention probably due to the decrease of bladder wall thickness. Closing incision of the bladder wall as four layers instead of three and / or delaying the catheter removal to fifth day may solve this problem. Complications of open prostatectomy ranged from 9.5% to 47.5% (12). It has been reported that complication rates in large series of TUR-P are as high as 18%. Most of these complications are related to hemorrhage or infection (6). However, Meier et al. compared their suprapubic prostatectomy serie with the large series of TUR-P reported by Mebust and associates. The overall early complication rate in the Mebust’s series is 25% and in Meier’s serie 19%. Mortality rates were similarly low, 0.2 % in the Mebust’s and 0 % in the Meier’s, and blood transfusion rates were 6.4% and 4.6% respectively. Carcinoma was identified in 22% of the Mebust’s serie and 9.6% of Meier’s series. The clot retention rate was higher (6.7%) in the Meier’s series than Mebust’s serie (3.3%) (6-12-13). In our study, early complication rate is 20.3 % and late complication rate is 14.3 %, and total complication rate is 34.6 %. Our total complication rate is not so different from the literature data (Tubaro et al.reported 31.2 % and Condi et al. reported 14 % complication rates). Overall complication rates for open prostatectomy was 34.6%, but our data is contained more detailed parameters. Our late and early complications were shown in Table 1. The mortality rates for both transurethral and open prostatectomies have decreased significantly in the past three decades (8-5) In most series the early mortality rate for TURP was 0.02% to 2.5% for TUR-P and 0.3% to5.8% for open prostatectomy (9-10) The ultimate goal of 0% mortality rate was achieved in our study. This low mortality rate was due to well patient care both preoperatively (especially in terms of respiratory and cardiac) and postoperatively (in terms of hemorrhage and comorbiditiy) also due to patient selection criteria. i.e. patients with serious cardiac problems were not accepted but transferred to another developed center. Preperitoneal inguinal hernia repair combined with urologic procedures have been reported with good success. (14-15) Simultaneous hernia repair appears as a safe procedure and may avoid a second surgical procedure. A total of 32 patients with inguinal hernia with BPH required only one access route. Although operating times were slightly increased, both problems were resolved at the same time. The blood transfusion rate in various series was between 1 % and 35 %. Condie et al. reported 1% blood transfusion rate, however, AHCPR revealed 35 % rate by a combined analysis of open prostatectomy series and approximately 15% of patients required blood transfusion (6-7-16). Transfusion rate was 10% in our series, ( 32 of 320 patients). The mean probability of developing urethral or bladder neck stricture is 7.7% ( 1.0-24.9%) (17). While in some cases no treatment was required, some patients have to undergo either dilation of the urethral stricture or bladder neck contracture, internal urethrotomy or a bladder neck contracture resection, under anesthesia (10-15). Five patients required dilatation and two patients required visual internal urethrotomy, in our cases. Urinary incontinence is defined as the involuntary leakage of urine. The review of the literature revealed 2.6%(0.5-7.2) stress incontinence and 0.3%(0.1-0.8) total incontinence following open surgical teratment for BPH (17). Our three patients had various degrees of prolonged incontinence, however the condition resolved completely within 3 to 5 months postoperatively. In coclusion, open prostatectomy for benign prostatic hyperplasia (BPH) is an acceptable option with a high degree of safety and efficacy in areas where the TUR-P equipment is lacking or this operation is technically impossible. REFERENCES
Copyright 2006 - Medical Investigations Society |

{kind=link}