 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
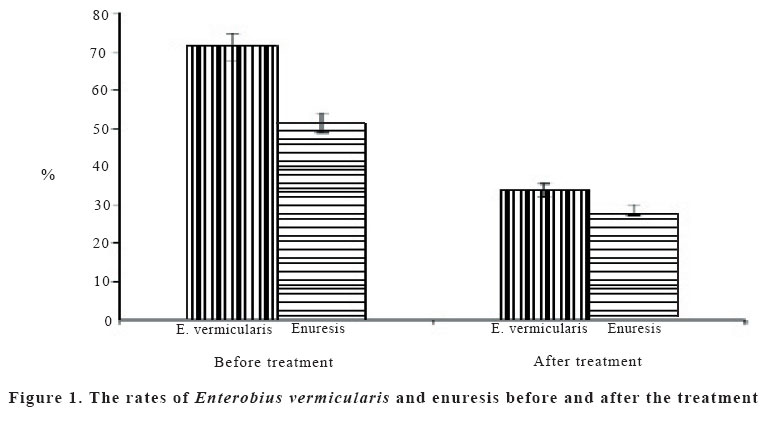
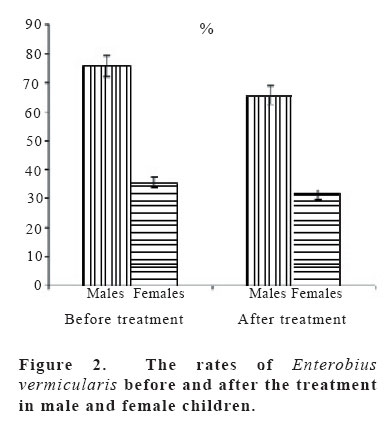
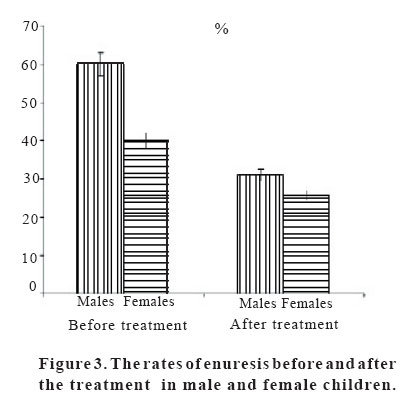
European Journal of General Medicine, Vol. 3, No. 1, 2006, pp.16-20 THE RELATIONSHIP BETWEEN ENTEROBIUS VERMICULARIS INFECTION AND NOCTURNAL ENURESIS Gülnaz Çulha1, Nizami Duran2 Mustafa Kemal University, Medical Faculty, Departments of Parasitology1 and Microbiology2, Hatay/Turkey Correspondence: Assistant Prof.Dr. Nizami DURAN Mustafa Kemal University, Medical Faculty,Department of Microbiolgy, Hatay/Turkey Tel: 903262141649, Fax: 903262144976 E-mail:nizamduran@hotmail.com Code Number: gm06004 Aim: The possible association between certain childhood infections and the propensity to develop nocturnal enuresis may include intestinal helminth infections. Objective: To explore the association between Enterobius vermicularis and nocturnal enuresis among children 4 to 7 years of age in a Turkish orphanage. Key words: Enterobius vermicularis, enuresis, pinworm, parasite, children. INTRODUCTION Nocturnal enuresis (bedwetting) is a socially disruptive and stressful condition which affects around 15-20% of children older than five, and up to 2% of young adults. Although there is a high rate of spontaneous remission, the social, emotional and psychological costs may be harmful. Enuresis is an important childhood problem that has been associated with a wide variety of child disorders, and with the socio-environment of the family (1,2). Intestinal helminth infections are more prevalent among the school-age children, especially preschoolers. In some groups, nearly 50% of children are infected. Infection often occurs in more than one family member. Adults are less likely to have pinworm infection, except mothers of infected children. Child care centers, and other institutional settings often more have cases of pinworm infection (3). Enterobius vermicularis (pinworm) is one of the most prevalent worms found in children worldwide. Pinworms, also called threadworms, typically infect the bowel of children in tropical areas (4,5). Enterobius vermicularis is the causative agent of human enterobiasis. The disease is more prevalent in temperate regions and is facilitated by factors such as overcrowding in schools and family groupings, as well as inadequate personal and community hygiene. (5). There are several drugs, which can help to eliminate pinworm. One of the most common drug is mebendazole. It is usually taken in a single dose or perhaps in two doses two weeks apart. The whole family must take the medication; otherwise it will not be very helpful. These drugs only kill the adult worms so attention to cleanliness is still extremely important. Petroleum jelly or anti-itch creams and ointments may be applied 2-3 times per day to reduce the itching that continues the cycle of infection (4,5,6). Urethral/vaginal reflux has been suggested as cause for enuresis. This concept is not widely accepted. Somewhat more realistic is the suggestion by Sachdev and Howards that a number of cases of secondary enuresis may be due to pinworm infestation (Enterobius vermicularis) (7). The association between enuresis and Enterobius vermicularis was reported in some studies (7-9). The prevalence of this problem as a cause of secondary enuresis is not clear at this time. However, it would seem practical to check all children with enuresis, especially girls, for pinworm infestation. In this study, we aim to investigate the frequency of Enterobius vermicularis, and its association with enuresis among children aged 4-7 years in an orphanage in Antakya. MATERIALS AND METHODS The current study was carried out in Antakya between March 2003-September 2003 to find the prevalence of enuresis and enterobiasis among children living in an orphanage in Antakya. For this purpose a total of 80 orphan children were included to this study. The mean age was 6.63±0.66 (range 4-7). The children were examined for Enterobius vermicularis infection using the cellotape anal swab technique. Nocturnal enuresis rates were investigated before and after mebandazole treatment in children with Enterobius vermicularis to search for the association. One tablet (>2 years; 100 mg PO bid for 3 d) was given as a single dose for the purpose of treatment. At the end of the treatment, perianal tape samples taken all of the children were examined. Data collection Firstly, a questionnaire about enuresis was constructed and data on this item was gathered. Data collection was done in cooperation with childrens’ nurse. Enuretic children’s nurses were interviewed on the frequency of enuresis during the day and night. Enuresis was defined as an unintended leakage of urine at least once a week in an individual old enough (older than 4 years) to maintain bladder control (10). Diurnal enuresis was defined as an unintended leakage of urine during waking hours and nocturnal enuresis was defined as bed-wetting in children older than 4 years at least once a week. Primary enuresis was defined as an unintended leakage of urine at least once a week in a child who had never had day or night bladder control for a period greater than 6 months. Secondary enuresis is considered when the child has been toilet trained for at least 6 months after the age of bladder control, and bladder control is subsequently lost (11). Statistical analysis The statistical analyses were performed by using Statistical Package for Social Sciences (SPSS, version 10.0) software. The chi-square test was used for statistical analysis. P values less than 0.05 were considered statistically significant. RESULTS The occurrence of Enterobius vermicularis was examined by perianal tape tests in 80 children. Total egg positivity rate for Enterobius vermicularis was 71.3% (57/80). The egg positivity rates for boys and girls were 75.6% (34/45) and 65.7% (23/35), respectively. Total enuresis rate was 51.3% (41/80), and 60% (27/45) of the boys and 40% (14/35) of girls had enuresis. After the mebendazole therapy, while the total egg positivity rate for Enterobius vermicularis was 33.8% (27/80), this ratio was 35.6% (16/45) for boys and 31.4% (11/35) for girls. There was a statistically significant decrease in the prevalance of Enterobius vermicularis after the mebandazole treatment in both boys and girls (P < 0.05). While before the mebendazole therapy, total enuresis rates was 51.3% (41/80), after the therapy it was found as 28.8% (23/80) in children (Figure 1). After the mebandazole treatment, the decrease of the enuresis rates in boys and girls was statistically significant (P < 0.05). After mebendazole therapy, while 16 (31.1%) of male children were positive for Enterobius vermicularis and 14 for enuresis, enterobiasis was found in 11 of female children and enuresis in 9 (25.7%). Statistically significant differences were found between the male and female children ((P<0.05), (Figure 2 and 3)). DISCUSSION Nocturnal enuresis is a common problem, affecting an estimated 5 to 7 million children in the United States and occurring three times more often in boys than in girls (12). Unfortunately, only about one third of the families of children with this frequently troubling problem seek help from a physician. Recent studies have provided more information about nocturnal enuresis, and generally effective treatment are available (1,2,12). It is known that intestinal parasites play an important role in the etiology of enuresis cases. It has been reported that enuresis was one of the shown symptoms in enterobiasis (7,8,13). In this study, we tried to determine the potential association between enuresis and Enterobius vermicularis in children. While before mebendazole therapy total egg positivity rates for Enterobius vermicularis was 71.3% (57/80), and 51.3% (41/80) of these children had enuresis, after the mebendazole treatment, a significant decrease of the prevalance of nocturnal enuresis (51.3%, 41/80) occured depending on the decrease of the prevalence of Enterobius vermicularis after the treatment (33.8%, 27/80), (p<0.05, Figure 1). Studies on the association between Enterobius vermicularis infection and nocturnal enuresis among children are limited in Turkey. In a study conducted by Erdemir et al (14), Enterobius vermicularis was present in 61% in the enuretic children (14). Also, they noticed that Enterobius vermicularis was the most frequent isolated microorganism among the enuretic patients (15). Similarly, from studies conducted in our country among the enuretic children, in the study of Tanyuksel et al (15), the rate of Enterobius vermicularis frequency was 31.3%, and, in the study of Yerel et al (16), it was 54% (15,16). In another study, Zeyrek et al (17), investigated the frequency of Enterobius vermicularis in 50 children with enuresis nocturna complaints among the ages 5-15. Enterobius vermicularis was identified in 33 cases (66%) in their sudy (17). With regard to studies from other countries, Otu-Bassey et al (13), investigated the prevalence of enterobiasis and its relationship with enuresis among 799, randomly selected children aged 5-14 years. In their study, compared with the egg-negative subjects, the 60 children who were egg-positive for Enterobius vermicularis were found to be much more likely to be suffering from enuresis (13). In one study, Kim et al (18), (1991) reported that the egg positivity rate of primary school children was 19.9% in Kangwondo province, especially 61.9% among orphan children and the egg positivity rate of different regions such as urban and rural areas was significantly different (18). These values (61.9%) are very close to the rates we have determined in our study (71.4%). It has been demonstrated that the occurrance of Enterobius vermicularis seroprevalence was 9% to 61% in the general population and the egg positive rate of different regions such as urban and rural areas was significantly different in our country and different places of the world (14-26). In the present study, egg positivity rate of Enterobius vermicularis was found to be higher than the finding conducted before in Turkey (14-17,19-22). This result may be explained that the children living in orphanage have low life standarts. In our study, the 71.4% Enterobius vermicularis prevalence found for orphan children approaches to the seroprevalence of Enterobius vermicularis prevalence reported by Kim et al (26). In conclusion, these results confirm an association between Enterobius vermicularis infection and nocturnal enuresis. We recommend that enuretic children should be screened for Enterobius vermicularis infection. Enterobius vermicularis infections are frequently seen in kindergarden, primary school and orphanage, where children are crowded, so hygiene should be provided adequately. In addition, the official personel of such should be educated about enterobiasis. In these places parasitic infections should be frequently screened. REFERENCES
Copyright 2006 - Medical Investigations Society |

{kind=link}
{kind=link}
{kind=link}