 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
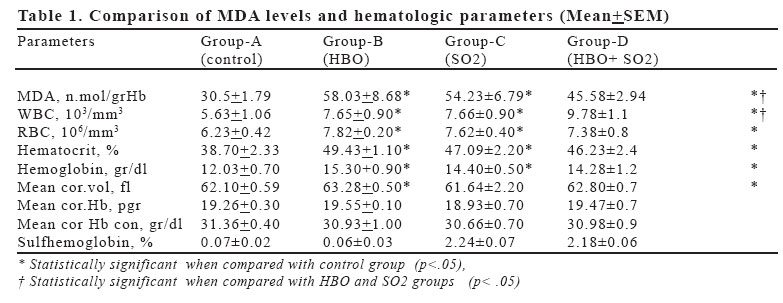
European Journal of General Medicine, Vol. 3, No. 1, 2006, pp. 21-28 THE OXIDANT EFFECTS OF HYPERBARIC OXYGENATION AND AIR POLLUTION IN ERYTHROCYTE MEMBRANES (HYPERBARIC OXYGENATION IN AIR POLLUTION) Özdal Etlik, Ahmet Tomur Gülhane Military Medical Academy, Department of Physiology, Ankara, Turkey Correspondence: Dr. Özdal Etlik Burc Molecular Genetik Tani ve Arastirma Laboratuvari Vali Konagi Cad. Orhan Ersek Sok. 19/2 34365 Nisantasi-Şişli, İstanbul, Turkey Tel: 902122919420, Fax: 902122472242 Code Number: gm06005 Aim: The aim was to investigate the interactions of hyperbaric oxygenation (HBO) and sulphur dioxide (SO2) inhalation (at 10 ppm, one hour daily for 45 days) on lipoperoxidation and fragility of RBC membranes. Key words: HBO, SO2, RBC, lipoperoxidation, fragility INTRODUCTION The increased O2 content of the blood caused by hyperbaric oxygenation (HBO) is very helpful in treating several diseases arising from or complicated by decreased tissue oxygen availibility (1,2). However, many researchers have reported that O2 in excess may have harmful effects. Lipid peroxidation due to free oxygen radicals (FOR) is known to occure during HBO (3-10). Peroxidation of membrane phospholid PUFAs (Polyunsaturated fatty acids) which is an important complication of HBO treatment (HBOT) was reported to lead to the disruption of the structural integrity of the membrane lipid bilayer and/or alter the boundary lipid microenvironment of membrane proteins especially those that maintain selective transmembrane ionic and potential gradients (11,12). Lipid peroxidation products accumulate in various tissues following hyperbaric hyperoxia and also depress the activity of Na-K ATPase (13-15). Lipid peroxidation, an autocatalytic free radical process, has been reported to have a very important effect in many diseases including various hemolytic anemias and hemoglobin disorders (16-18). Air pollution is a very important problem which continues to threat human health for a long time all over the world. Some of the major air pollutants are sulphurdioxide (SO2), carbon monoxide, nitrogen dioxide (NO2) and ozone (O3). SO2 is reported to cause an increase in the daily number of deaths due to respiratory and circulatory system diseases. SO2 is absorbed readily (99%) through the respiratory tract and shows a wide tissue distribution. The amount of SO2 in blood and other tissues increases proportionally with it’s concentration in the inhalation air. Radioactive sulphur (S35) can be detected in the protein structures of tissues at least for one week (19-21). Haider et all. reported an increase in the lipid peroxidation of the lungs and heart of the rats due to SO2 inhalation at 10 ppm 1 hour daily for 30 days (22). Significant increases in sulfhemoglobin ratios and RBC activities of superoxide dismutase and glutathione peroxidase during an heavy air pollution were determined in an epidemiological study (23). Higher sulfhemoglobin and osmotic fragility ratios, WBC and RBC counts, hematocrit and hemoglobin values and lower erythrocyte deformabilities induced by SO2 inhalation were detected in various studies (24-28). Morever, the inhalations of various air pollutants (NO2 O3, cigarette smoke) were reported to result in higher MDA levels and osmotic fragility ratios (29-40). The aims of the present study firstly, was to investigate if HBOT caused an increase in the formation of free O2 radicals in RBC membranes. Secondly, since HBOT is administered all over the world including many cities with a serious air pollution problem, it was investigated if there were any adverse effects on RBC membranes in HBO treatments during heavy air pollutions. MATERIALS AND METHODS Animals and exposures. A total of 24 rats (Swiss-Albino, male, weighing 214-222 gr.) were divided into four groups by “Simple random sampling method” as follows: Group-A (n:6): control, group-B (n:6): HBO, group-C (n:6): SO2 and group-D (n:6): HBO+SO2 Groups B and D exposed to HBO in a cylindirical pressure chamber under 3 Atm abs 303.9) pressure, 1 hour daily for 45 days. A dish with sodalime and sicca-gell spheres were placed in the chamber to prevent CO2 accumulation and an increase in humidity. Pressurisation was supplied with compressed O2 from commercial cylinders. The pressure was increased beginning with a slow initial phase of 1 ATA/30 s. and then doubled every 30 s. according to a previously validated schedule (41). SO2 were applied in groups C and D in a specifically designed exposure chamber at 10 ppm (MAC: Maximum acceptable dose), 1 hour daily, for 45 days. The flow rate of air containing SO2 was 30 L/min. SO2 concentration of the chamber air was measured by H2O2-acid titration method. Ambient air was applied at a similiar flow rate under the same conditions (1 hour daily, for 45 days) in groups-A (control) and B (HBO) (22). Heparinized blood specimens were obtained by cardiac puncture under ketalar (20-40 mg/kg) + xylasine (4-8 mg/kg) anesthesia at the end of the inhalation period. All the studies were completed in 4 hours. Animals were supplied with standart rat chow and tap water. Minimal numbers of animals were sacrificed for ethical purposes. Hematological measurements. RBC and WBC counts, hemoglobin, hematocrit, mean cell volume, mean corpuscular hemoglobin and mean corpuscular hemoglobin concentration values were determined using an electronic hematology analyzer (Coulter counter model S plus VI). The extent of lipid peroxidation was determined by measurement of MDA levels according to the method of Stocks and Dormandy (42,43). Reagents. (1) Buffered saline: 17.6 ml 0.5 M KH2PO4 + 60.8 ml 0.5 M K2HPO4 were made up to 1 liter with deionized water. An aliquot of this solution (100 ml) was added to 1 liter 0.15 M NaCl, pH 7.4 (2) TCA-Arsenite solution: 280 g trichloracetic acid (TCA) were added to 500 ml deionized water followed by 13 g Na-arsenite. The mixture was dissolved by heating, then cooled. Finally, it was made up to 1 liter with deionized water and filtered. (3) TBA solution: 5 g thiobarbituric acid (TBA) was dissolved by heating in 200 ml deionized water together with 25 ml, 1 N NaOH. The solution was cooled and made up to 500 ml with deionized water and filtered. Procedure: Fresh blood obtained by cardiac punction was centrifuged. The plasma and buffy coat (the layer composed of leukocytes and thrombocytes) were aspirated. Erythrocytes were washed with 50 volume of P-tampone and centrifuged twice. Hemoglobin concentration was measured by adding 0.02 ml of blood to 5 ml Drapkin solution, shaking well, waiting and reading the absorbance value at 540 nm spectrophotometrically (Shimadzu UV-120-01). Afterwards, Hb concentration was brought to 3 gr/100 ml by adding P-tampone. 3 ml of the cell suspension was added to 2 ml TCA-arsenite solution. The mixture was centrifuged, 3 ml of the supernatant was transferred to a 15 ml centrifuge tube and 1 ml of TBA solution was added. An air condenser was fitted to the tube and the mixture was incubated for exactly 15 min in a boiling-water bath. The tube was cooled with tap water immediately. The absorption spectrum of the mixture between 500 and 600 nm was plotted by using a spectrophotometer. The formula (OD 532-600) x 900 gave the MDA concentration in n-mol/g Hb. Osmotic fragility measurements were done spectrophotometrically by using heparinized blood (44). Results were expressed as mean + standart error and the groups were compared by Mann/Whitney U-Wilcoxon Rank Sum W test. RESULTS Lipid peroxidation (Table 1). The extent of lipid peroxidation of RBC membranes in groups B, C and D were significantly higher than in control group (p<.01). Marked decreases in MDA levels were observed in group D compared with groups B and C (p<0.05). Osmotic fragility ratios (Figure 1). The results obtained in group B and C at concentrations of 0.30%, 0.40%, 0.45%, 050%, 0.55%, 0.60% were significantly higher than in group-A (p< 0.05). The values of group D were significantly lower than in group B at concentrations of (0.30%, 0.40%, 0.45%, 0.50%, 0.55%, 0.60%, 0.70%) (p< 0.05) and lower than in group C at concentrations of (0.45%, 0.50%, 0.55%, 0.60%, 0.70%) (p<0.05). However, results of group D were also significantly higher than in group-A at concentrations of (0.40%, 0.45%, 0.50%, 0.55%, 0.60%) (p< 0.05) . Hematologic parameters (Table 1). WBC counts in all of the groups were significantly higher than in control group (p< .05). The results of group D were significantly higher than in groups B and C (p< 0.05). RBC counts, hematocrit and hemoglobin values in all of the groups were significantly higher than in control group (p< 0.05) and no statistically significant differences were determined between the other groups (p>0.05). No significant differences in MCV, MCH and MCHC values were detected between the groups also (p>0.05). DISCUSSION Five important features of erythrocytes have caused them to be prefered extensively as a model for investigating oxidant stress: 1) RBCs are always in contact with molecular O2 directly. 2) They contain metal ions catalysing oxidative reactions. 3) RBC membranes have got plenty of PUFA (polyunsaturated fatty acids) which is susceptible to lipid peroxidation. 4) They do not have ability to repair membrane damages and regenerate. 5) They circulate in the plasma which is poor in antioxidant enzymes such as superoxide dismutase, glutathione peroxidase and catalase (45). Therefore, erythrocytes may be accepted as an useful and convenient cell system in which to evaluate the effects of HBO administered in therapeutic situations or in alternate environments (e.g. deep sea diving) (46). In recent years, oxidant stress related damages of biological systems have been attracting a growing interest of researchers. FOR cause oxidant-induced changes in the structure and function of erythrocyte membranes. Major changes reported by different researchers are lipid peroxidation, membrane protein-crosslinkings and oxidation of heme proteins resulting in their crosslinkings to skeletal proteins, i.e spectrin, actin, cytoplasmic component of band 3 (47-50). Free oxygen radicals induced changes result in severe deteoriation of membrane structure and function causing increases in osmotic fragility ratios, accelerated cell aging and premature cell death ultimately. The susceptiblity to auto-oxidation is greatly increased in many haemolytic diseases and hemoglobin disorders and the oxidation of lipids are known to lead to cell death inevitably . In this study, increased RBC counts, hemoglobin and hematocrit values as in the previous studies were also determined in groups B, C and D (25,26,27,51,52,53,54). These changes may be due to one of the followings: decreased plasma volume related with increased vascular permeability induced by free oxygen radicals, erythropoetic effect of fragmentation products of highly fragile erythrocytes or splenic contraction due to anesthesia complication resulting in RBC release or functional anemia due to sulfhemoglobinemia (for groups C and D) or decreased plasma volume related with increased vascular permeability induced by the irritant effect of SO2 (for groups C and D) (41,55,56,57,58,59,60). Since no differences in hemoglobin, hematocrit and RBC counts were determined in group D compared with group C, these findings indicate that increases in these hematological parameters are not directly related with oxidant stress. Probably, these increases, also determined in group D, are related with the other factors mentioned above. MCV values in group-B were found significantly higher than in the control group. Highest osmotic fragility ratios determined in this group may be evaluated as a result of increased MCV values. Higher WBC counts in groups B, C and D than in control group were also determined as in the previous studies. Activated neutrophills are known to release reactive O2 species causing oxidant damage in blood and the other tissues. This increase which is known to be a response to the oxidant damage may have contributed to lipid peroxidation and structural and functional changes in erythrocyte membranes (63-63). But, while MDA levels in group D is lower than the groups B and C, WBC levels is significantly higher than the groups B and C, so the importance of the contribution of WBC to the lipid peroxidation must be very little or WBC increase must be related with another unknown factor. We determined in this study that HBO and SO2 exposures resulted in an increase in MDA levels which is known to cause hemoglobin denaturation, membrane lipid peroxidation, cross-linkings between membrane skeletal proteins and between membrane and hemoglobin. Increases in osmotic fragility ratios due to structural and functional membrane damage were also observed in both HBO-treated group and SO2-inhaled group. The changes following HBOT may be related with various free oxygen radicals and the other changes obtained following increased sulfhemoglobinemia induced by SO2 inhalation may be due to sulfur dioxide anion radical (SO2-) which was reported to form via one electron transfer resulting in the reduction of SO2 to SO2- by cytochrome P-450 (64). MDA levels were significantly lower in group D than in groups B and C. Morever, significant decreases in osmotic fragility ratios were observed in group D compared with the same groups. This finding may be evaluated as a result of the presence of sulfur dioxide anion radical under the anaerobic conditions only. This radical can not be detected in the presence of air (65). The sulfur dioxide radical metabolite may be produced under aerobic conditions, but subsequently react with oxygen. The air oxidation of this free radical (to form superoxide and regenerate (bi) sulfite) occurs with a rate constant of 4.1 x 103 M-1 sec-1 (65). Moreover, since rat hepatic microsomes in the presence of NADPH will reduce molecular oxygen to superoxide, (bi)sulfite and oxygen may be reduced at the same site(s) (66,67). If oxygen is the better electron acceptor, it could prevent the reduction of (bi)sulfite by competitive inhibition (51). Therefore, as a conclusion, these findings indicate that the combination of SO2 and HBO can reduce lipid peroxidation and oxidant damage in erythrocytes induced by free O2 radicals or at least, this combination does not cause an additional radical damage. REFERENCES
Copyright 2006 - Medical Investigations Society |

{kind=link}
{kind=link}