 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
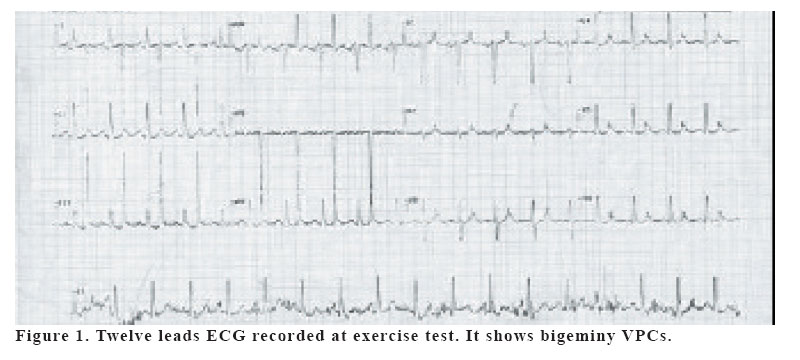
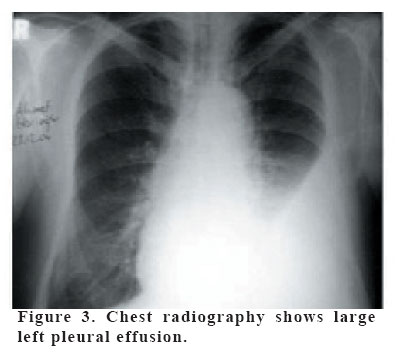
European Journal of General Medicine, Vol. 3, No. 1, 2006, pp. 29-31 INTERPOLATED BIGEMINY VENTRICULAR PREMATURE CONTRACTIONS DUE TO CARDIAC COMPRESSION OF LEFT PLEURAL EFFUSION: A CASE REPORT Aydın Akyüz1, Cenap Özkara2, Niyazi Güler3, Hasibe Özkara1 Çorlu Sifa Hospital, Departments of Cardiology1 and Cardiovascular Surgery2 Tekirdağ, Yüzüncü Yıl University, Medical Faculty, Department of Cardiology3, Van, Turkey Correspondence: Doc. Dr. Niyazi Guler Yüzüncü Yıl Ü. Tıp F. Araştırma Hastanesi, Van, Türkiye Fax: 904322168352, Tel: 905323736689 E-mail: niyaziguler@hotmail.com Code Number: gm06006 We described interpolated bigeminy ventricular premature contractions due to cardiac compression by a large left pleural effusion during exercise test. A 68-year-old man was admitted to the hospital for further examination of chest oppression. His history included a rheumatoid arthritis for more than 20 years and multiple admissions to the hospital. He had been on indomethacin (75 mg/daily) in partial remission for more than 1 year. Laboratory findings of thoracentesis fluid revealed that the cause of pleural effusion was rheumatoid arthritis. He had no diabetes mellitus, thyrotoxicosis, myopericarditis, ischemic or valvular heart disease. Key words: Pleural effusion, ventricular premature contraction, exercise test. INTRODUCTION The seen of bigemine ventricular premature contractions (VPC) is important sign of electrocardiogram (ECG) since ventricular fibrillation may begin in these patients. Although bigemine VPCs are occurred in patients with cardiac disease, it may develop due to extracardiac diseases such as anemia or tiroid disorders. In this paper, we present a case with exercise induced VPCs, which is probably due to the cardiac compression by a left pleural effusion. CASE A 68-year-old man was admitted to our hospital with complaints of retrosternal pain and shortness of breath. Physical examination revealed decreased breath sounds in the left hemithorax. Percussion of the lung revealed dullness with absent tactile fremitus over the area. His physical examination was otherwise unremarkable. His history included a rheumatoid arthritis for more than 20 years and multiple admissions to the hospital. He had been on indomethacin (75 mg/daily) in partial remission for more than 1 year. He underwent a treadmill exercise test for the evaluation of myocardial ischemia. Baseline ECG showed mild sinus tachycardia with QTc of 320 ms. Exercise test was terminated in the 20th second of exercise because of arrhythmia. The second beat in D1 lead, and each alternate one following it, is a ventricular ectopic premature beat (Figure 1). Arrhythmia in a form of premature ventricular contractions (PVC) of bigeminy types continued for about 1 minute. The VPCs in this case were of R–on-T type (Figure 2). Blood pressure and oxygen saturation were normal. Serum electrolytes, CK-MB, troponin T, C-reactive protein, and hemogram, measured on the first day of the exercise test were all within a normal range, apart from leukocyte a count of 11.500. Chest radiography showed large left pleural effusion (Figure 3). A yellow-green color was seen in thoracentesis fluid. The fluid was an exudate with low glucose (19 mg/dl) and high LDH. The complement level was low, with high titers of rheumatoid factor. Echocardiography revealed that systolic and diastolic left ventricle functions were normal. We also could not discern any pericardial effusion on echocardiography. To exclude myocardial ischemia, coronary angiography was performed and it revealed normal coronary arteries. DISCUSSION The present report showed an association between interpolated bigeminy VPCs and pleural effusion during exercise test in a patient with rheumatoid arthritis. An example of a VPC occurring very early and being “interpolated” as a result of this marked prematurity is seen in our case. Because the R wave of the ectopic beat begins before the T wave of the preceding non-ectopic beat is completed, the premature beat is said to be of the “R–on-T” type in our case. VPCs had identical morphology, indicating that they were unifocal ventricular ectopic beats. They also had the same coupling interval and they were therefore likely to arise on the basis of a re-entry mechanism. In our case, exercise induced VPCs were probably due to the cardiac compression by a left pleural effusion. Although another cause of the VPCs might have been silent myopericarditis due to rheumatoid arthritis, the signs of myopericarditis were not seen on the echocardiography. In addition to normal echocardiographic findings, cardiac enzymes such as CK-MB, LDH, and troponin were within normal ranges. Although the effects of pleural effusions on the ECG have been known, to our knowledge, there are no data in the literature about an association between bigeminy VPC and large pleural effusions. Manthous et al reported a case of a patient with extreme QRS axis deviation mimicking acute myocardial infarction (1). Thoracentesis in this case caused the return of a more normal axis. With the presence of a large left pleural effusion, the frontal plane QRS axis may be shifted to the right. An experimental study investigated ECG findings of patients suffering from large left pleural effusion (2). And this study demonstrated the QRS amplitudes were decreased to significant level at large effusions (2). Tursi et al reported that the compression of the heart with retrocardiac stomach provoked the VPCs in the absence of cardiac disease (3). Similarly, the increase in direct or indirect pressure exerted on the global surface of the heart seems to be the cause of the bigeminy VPCs observed in our patient. REFERENCES
Copyright 2006 - Medical Investigations Society |

{kind=link}
{kind=link}
{kind=link}