 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
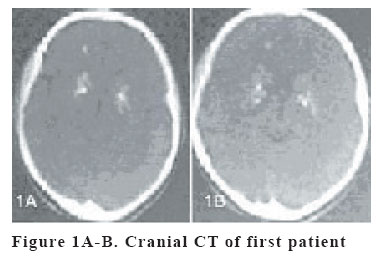
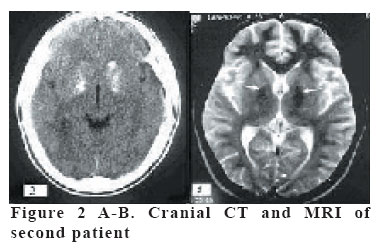
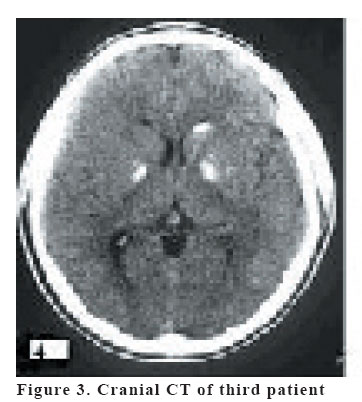
European Journal of General Medicine, Vol. 3, No. 1, 2006, pp. 35-40 FAHR SYNDROME Three cases presenting with psychiatric signs Murat Gülsün1, Ali Fuat Baykız 2, Serdar Kabataş3, Hasan Belli4 Tatvan Military Hospital, Psychiatry Clinic, Bitlis1, Elazığ Military Hospital, Psychiatry2 and Neurosurgery3 Clinics, Psychiatry and Neurology Hospital Psychiatry Clinic4 Elazığ, Turkey Correspondence: Murat Gülsün, MD, Elazığ Asker Hastanesi, Psikiyatri servisi,Elazığ Türkiye E-mail: mgulsun@yahoo.com Code Number: gm06008 Fahr syndrome, a clinical entity that manifests with various signs and symptoms and has a familial predisposition is characterized by symmetric calcification of basal ganglia. It may present with neuropsychiatric, extrapyramidal and cerebellar symptoms. The etiology has not been defined yet. Three cases of Fahr syndrome; presenting with various clinical signs and psychiatric symptoms are reported in this article. The first case that occured following Brucella treatment and the other two occuring idiopathically are evaluated with a neuropsychiatric approach. Key words: Fahr syndrome, basal ganglia, calcification, Brucella, anxiety, psychosis INTRODUCTION Fahr disease has been described for the first time by Fahr in 1930. The clinical course of the disease has a degenerative component. There may be mental and motor disability which accompanies epileptic syncope, increased neuromuscular excitability and tetany, paresthesia, intracranial calcification and cataract. The mineral deposition may lead to cell loss in the cerebral cortex, basal ganglia, dentate nucleus and subthalamus (1). In CT of 2318 patients with Fahr disease 12.5% have calcifications in basal ganglia. The most frequently seen localization is globus pallidus with a rate of 96.4% (2). The calcifications are probably due to lipid deposition and demyelinization. The disease is characterized by symmetric calcifications of dentate nucleus and white matter. It may present with different clinical aspects. The etiology is not clear although many researches have been done. The trials which has been performed with cases of familial predisposition point out that there may be an autosomal recessive transition (3). In the etiology metabolic diseases, (hypoparathyroidism, hyperparathyroidism), mitochondrial cytopathy, infectious diseases; Epstein Barr Virus infections, tuberculosis and AIDS may play a role. Neuropsychiatric, extrapyramidal and cerebellar symptoms, convulsive seizures, Parkinson like symptoms; dementia and speech disorders may accompany the clinical picture (4-6). There are also cases reported without neurologic signs. It usually appears between 40-60 years of age. However it may also be rarely seen in children. Chorea- athetoic movements are more common in the childhood period while progressive mental disorders take place in the adulthood. Cummings et al. (1983) have described two psychiatric symptoms in basal ganglion mineralization; cases with psychiatric symptoms appearing in the early period (mean 31 year) and in late period (mean 49 year). Motor and cognitive symptoms in cases with basal ganglion mineralization which appears in the late period are more significant (7). Pallidal lesions may cause disorders related to motivation, judgement and insight in humans. Idiopathic basal ganglia calcification may lead to various neuropsychiatric symptoms. Patients with basal ganglia calcification present initially with psychiatric symptoms. When psychosis occurs in Fahr’s disease, it usually presents in persons 20–40 years of age as part of the so-called early adult-onset Fahr’s disease. Classic schizophrenia-like symptoms have been described, including auditory hallucinations, paranoid delusions, delusions of reference, and catatonia. Psychotic symptoms that are not typically associated with schizophrenia have also been described, including musical auditory hallucinations and complex visual hallucinations (8). Neurologic symptoms in older cases are more distinctive than early period cases. The localization of the calcifications is not always consistent with the neurologic signs. In diagnosis, CT is found to be more functional than MRI. In this article three cases of Fahr syndrome; one after Brucella treatment and the other two occuring idiopathically presented with different clinical signs and psychiatric symptoms were evaluated with a neuropsychiatric approach. CASE I She is a 14 year-old girl who was born via vaginal route to a healthy mother and father as a fifth child. She was graduated from a primary school and was diagnosed with Brucella two years ago and received Streptomycine for one month and in her second month of therapy, because of periodic tetany of her fingers starting as seizures she was given high dose analgesics, but there was no acceptable relief in her complaints. She has entered into a period characterized by perturbation, uneasiness, irritability, expectation anxiety, choking sensation while breathing, and discomposure and tension type headaches. The contractions appear to be more frequent when her anxiety increases and decrease when her anxiety level is lower. With these complaints the family admitted to a pediatrician. As the tetany increased with the increased anxiety, she was referred to a psychiatric outpatient clinic with a prediagnosis of conversive reaction. At the initial admission the case was not in a significant tetanic condition, but during her physical examination she started to breath deeply and in a few minutes she had tetany in her fingers of her both hands. It was thought that the clinical picture was due to alcholosis developing because of the hyperapnea; so slow and rythmic breathing and relaxation exercises were tried in order to get CO2/O2 balance. In that period the tetany was partially controlled. The neurologic examination was evaluated as normal. Laboratory findings; free T3, T4, TSH, brain MRI, whole blood count, sedimentation, routine biochemical tests were within normal limits. Serum calcium result was 7,1 mg/dl (normal: 8.8-10.2), Serum intact PTH value was : 60 pg/ml. EEG findings were within normal limits. Radiological findings: in Figure 1A-B; Cranial CT demonstrates that there are millimetric and almost symmetric calcifications in both frontal lobes at the level of basal ganglia in the axial sections through the basal ganglia and lateral ventricules. Mental State Examination; The case; who appeared to be the same as her chronologic age was socially limited and her mood was agitated and anxious, she had a good self care and normal speech pattern and her interest to her environment was evaluated to be normal. The periodic tetany which augmented with the increased anxiety was seen in fingers of her both hands. Her sleep and appetite was diminished, her miction and defecation routine was normal. Her memory, perception, orientation and attention were within normal limits. Quantitative and qualitative judgement was normal. Her emotional state was distorted as anxietic, her thought content was focused on the preoccupation of her illness, and her conduct was anxietic and disturbed. Pscyhometric Evaluation: She got a score of 30 in Hamilton Anxiety Rating Scale (9). In Psychiatric Evaluation according to DSM IV anxiety disorder due to general medical condition was diagnosed (10). In the treatment Fluoxetin 20mg/day and Vitamine C (Ascorbic asit) 1000mg, Calcium carbonate 625 mg, Vitamine D3 (Cholecalsiferol) 300 IU, Vitamine B6 (Pyridoxine) 15mg combined preparation was started. In her 14th day of treatment a decrease in the frequency of her tetanic spasm was observed. In 20th day there was an increase in her tetany and the serum calcium levels decreased to 6.2. Therefore according to the consultation with the pediatric clinic; combined calcium and vitamine complex preparation was stopped and calcitriol 0, 25 mcg every other day was added. The case is using Fluoksetin 20 mg/day and 0, 25 mcg calcitriol for one month and her calcium level is 9.9 mg/dl. At the end of her first month she regressed to 10 points in Hamilton Anxiety Rating Scale. There is a significant improvement in her general medical condition. CASE II He is a 27 year old, married, government official, who is working for 6 years. While he had no need to seek psychiatric help before, he had admitted to our clinic for he had lost his joy of living and have complaints such as insomnia, loss of appetite, feeling himself in a gap, weakness, loss of energy, loss of enthusiasm in his work, feeling of failure, feeling as if something is being taken out of his chest and sometimes hearing murmury sounds for the last 2 months. He was thinking of suicide especially for the problems he was challenged in his work place. He was married six months ago and he had troubles in establishment of harmony. He had no significant ilness in his family and personal history. He was hospitalized and followed up in the psychiatric clinic because of his suicide risk. In his hospitalization period neurosurgical and internal medicine consultations were performed. In mental state examination; he was standing, looked the same as his age, his self care and his interest to his environment was diminished, his mood was calm, mimics and gestures were appropriate with his mood , his socialibility was eligible for a relationship, introverted and his sleep and appetite level was decreased. He was concious, his attention was decreased, his memory was hypoamnesic, his perception was distorted because he had hearing type hallucinations and his orientation was limited to his illness. His intelligence and judgement was adequate. His rate of flow of the thoughts was slow, but arrives to a target, in his thought content he had pessimistic ideas about his future. His affect was increased as distressed and distorted as anxiety. In his behaviour there was a pscyhomotor retardation, social withdrawal and the feeling of failure. In his neurologic examination there was no abnormal finding except postural tremor. As the CT scanning revealed calcifications in the bilateral basal ganglia (Figure 2A) cranial MRI was obtained and in MRI scanning at the level of basal ganglia, bilateral T2 weighted axial cross sections there was hypointense areas consistent with calcifications (Figure 2B). EEG and sleep deprived EEG results were evaluated as normal. Whole blood count, whole urine analysis, sedimentation rate, fasting blood glucose, renal function tests, liver enzymes, lipid profile, T3, T4, TSH levels, ceruloplasmine, serum copper, serologic tests (C3, C4, antinuclear antibody, romatoid factor) blood calcium and parathormon levels were within normal limits. In Neuropscyhometric Evaluation; the case got 30 points in Hamilton Depression Scale (The Hamilton Depression Rating Scale; HAM-D; scores between 7 and 17 indicate mild depression, scores between 18 and 24 indicate moderate depression, and scores over 24 indicate severe depression. (11). MMPI (Minnesota Multiphasic Personality Inventory) resulted as; ‘’the profile is not accountable. The F scale could not be evaluated as T score. Depression and psychotic subscales are increased in clinical subscales.’’ In his treatment fluoxetin 20 mg/day, alprozolam 2 mg/day and olanzapin 10 mg/day was started. In his 6 weeks hospitalization period although he received antidepressive and antipsychotic treatment there was no progression in his complaints. Therefore; his fluoxetine dose was increased to 40 mg/day, and olanzapinin dose to 15 mg/day and mirtazapine 30 mg/day was added to his treatment. In his next 1 month period no improvement in his clinical picture could not achieved. He was referred to a training hospital for further investigation and they suggested continuing of the existing treatment and was hospitalized in the same clinic again. After 2 months of antidepressive and antpsychotic treatment, his The Hamilton Depression Rating Scale (HAM-D) score regressed to 23. In his next follow-up, it was observed that he has stopped his drugs and had dizziness. He was hospitalized again and for his treatment as venlafaxine 75 mg/day, olanzapin 15 mg/day, mirtazapin 30 mg/day and buspiron 15 mg/day were used. Venlafaxine dose was gradually increased to 225 mg/day in two weeks period. Although there was a reduction in his depressive complaints the psychotic course and the dizziness was continuing. The patient is still following. Radiological examination and the organic etiology was planned to be reevaluated. CASE III He is a 23-year-old, single man who is in trade business. He has been diagnosed with “Psychotic Disorder (Paranoid Type)” and receiving 15mg/day haloperidol and 4mg/day biperiden treatment for 3 years. Although he was hospitalized twice for short periods, he was discharged on the demand of his family to be followed up by the outpatient clinic. He was taken to hospital by his family due to complaints including self care deterioration, hearing voices of criticism, locking himself in his house because of the thoughts of being injured by other people. The patient was hospitalized because of his intensive homocide and suicide thoughts. In his hospitalization period neurosurgical and internal medicine consultations were performed. In his psychiatric and neurologic examination; the patient was standing and looked like in his age. His selfcare was decreased and his interest to his environment was lessened, his mood was anxietic, suspicious and his mimics and gestures were consistent with his mood. His socialibility was limited but was eligible for a relationship. Although he was not very talkative, his tone of voice was increased. He was concious, his attention was slightly decreased, and his attentional functions were within normal limits. His perception was distorted as he had hearing and visual hallucinations. His orientation to his illness was distorted. Although his intellegence was clinically adequate his judgement and insight was deterioriated. His sleep and appetite was reduced and his flow of thoughts was slow but arrived to a target. In his thought content there were grandiose and paranoid delusions. His affect was indifferent and in his behaviour during the interview there was an anxietic, restless, suspicious appearence. According to anamnesis obtained from the family he was agitated and agressive, there was a reduction in his functions and he had insomnia. In his neurologic examination there was no abnormal finding except postural tremor. In cranial CT, it was seemed that there were symmetric calcifications in both frontal lobes at the level of basal ganglia in the axial sections through the basal ganglia and lateral ventricles (Figure 3). Whole blood count, whole urine analysis, sedimentation rate, fasting blood glucose, renal function tests, liver enzymes, lipid profile, T3, T4, TSH levels, ceruloplasmine, serum copper, serologic tests (C3, C4, antinuclear antibody, romatoid factor) blood calcium and parathormon levels were within normal limits. In Roschach test: ‘’the psychogram could not be developed because of inadequate answers.’’ In MMPI: ‘’There was distortion in ego functions, strong depression, immaturity, impulsivity, reference ideas and persecutation delusions.’’ The patient was hospiatlized and his treatment was started. His haloperidol dose was reduced and his olanzapine dose was gradually increased to 15 mg/day. While his Brief Psychiatric Rating Scale (BPRS) score was 49 at his admission, after 3 weeks olanzapine treatment it regressed to 35 points (12). However his intense paranoid delusions were continuing. Olanzapine dose was increased to 30 mg/day and Valproic asid 1000 mg/day was added to the treatment. After 8 weeks of treatment the BPRS scale score were 28. DISCUSSION In case-1 Cranial CT demonstrated that there are millimetric and almost symmetric calcifications in both frontal lobes at the level of basal ganglia in the axial sections through the basal ganglia and lateral ventricules. In the literature it was reported that in Fahr disease there are symmetric calcifications in the white matter of cerebral hemispheres, basal ganglia and cerebellum (13). The findings of the cranial CT of the case are consistent with the Fahr disease. In our case the tetany occurs usually in periods when her anxiety increases. When she has anxiety, her breathing increases and causes respiratory alcholosis which leads to deeper hypocalcemia. While her anxiety level is lower the hypocalcemia continues, but it is observed that she is partially able to manage this. Therefore; in a condition in which hypocalcemia occurs due to hyperventilation developing because of anxiety; antidepressive drug use may cause positive effects. The progression in our case may possibly be due to the oral calcium preparations which correct the general medical condition of the patient. However the existing picture was characterized by painful tetanic contractions which significantly detoriates the general medical condition of the patient and as her quality of life was negatively effected, the antidepressive treatment was decided to be stopped and just the follow up of the changes in clinical picture was determined because of ethical considerations. In literature Fahr disease may present with dementia, chorea-atetoid movements, and psychotic and demantial forms and there may not always be a relationship between the lesion and the clinical appearence. In case-I, there is no cognitive function destruction, dementia or psychotic disorder as mentioned in the literature. While periodic tetany may be seen in the upper extremities, the extrapyramidal system findings are within normal limits. It is difficult to explain the anxiety with lesion-clinical compatibility perspective. It seems to be more logical to interprete the anxiety secondary to painful tetanic contractions that disrupts the patient’s functionality. In Fahr disease’s etiology infection diseases; especially Epstein Barr Viruse infections, tuberculosis and AIDS may play a role (14), but as in the literature there is no case reported secondary to Brucella disease, it makes it worth to point it out. In our case the tetanic contractions due to hypocalcemia occurs one month after the Streptomycine administration which she was given for Brucella infection. Brucella infection invading the brain tissue is rarely reported in the literature (15). There is no case reported secondary to Brucella disease in the literature; therefore it is worth reporting. It is difficult to answer the questions whether the Fahr syndrome was triggered by Brucella infection or if it is a condition due to neurotoxic effects of Streptomycine. However, the case was evaluated as highlighting the etiologic investigations of Fahr syndrome. In cases II and III a significant etiologic factor could not be found. However it is important to point out that both of the cases present with psychotic signs. In the organisation of basal ganglia there are pathways travelling from cerebral cortex to ‘’patch’’ and ‘’matrix’’ regions of the striatum. ‘’Patch’’ region is more related to limbic region and the functions are not specific. ‘’Matrix’’ is found to be more specific and related to sensorymotor functions (16,17). It is reported that in basal ganglia thalamocorticostriatal damage may trigger schizophrenia-like syndrome. In this group, as neurologic signs, extrapyramidal syndromes, epileptic seizures and coma may be seen and cognitive disfunctions, mood disorders and psychotic symptoms may accompany the clinical picture . In a research it was reported that there is a close relationship between the depressive disorder and the basal ganglion calcification (18). Chiu and colleagues reported a case with a delusionel disorder and tardive diskinesia related to basal ganglia calcification (19). There is no familial predisposition in three of the cases. The common features seen in all three cases are having psychiatric symptoms, resistance to treatment when there is a psychiatric component and presenting as an acute onset illness. In Fahr Syndrome there may not be a correlation between the lesion and the clinical signs. However, as basal ganglia and especially putamen and limbic structures have close organisation, it may be thought that the psychotic component may be related to basal ganglion calcification. Although all three cases have similar basal ganglion lesion, in the first case there is no lesion-clinical signs correlation as she did not have a psychotic component. As she is only 14 years old it is possible to see the psychotic signs in the long run. As there are different clinical manifestations in all of the three cases, cognitive dysfunctions, mood disorders and psychotic symptoms are expected. In the onset of the disease psychiatric symptoms are usually more prominent than the neurologic symptoms. From this point of view it is important to investigate the organic etiology in the resistant cases to the treatment. Lauterbach and colleagues reported that in two cases with cognitive dysfunction, symptoms like temporal lobe lesions were seen. 9 In the neurologic examinations of the last two cases as there is extrapyramidal component and temporal lobe originating symptoms like hearing hallucinations it was thought that the clinical state may be related to pallidal lesions. Attributing psychiatric symptoms, including psychosis and anxiety disorder to basal ganglia calcification in Fahr’s disease remains debatable. However, in these cases, it was shown that basal ganglia calcifications may lead to various neuropsychiatric symptoms. REFERENCES
Copyright 2006 - Medical Investigations Society |

{kind=link}
{kind=link}
{kind=link}