 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
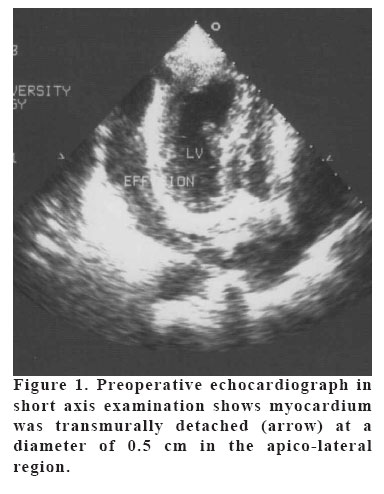
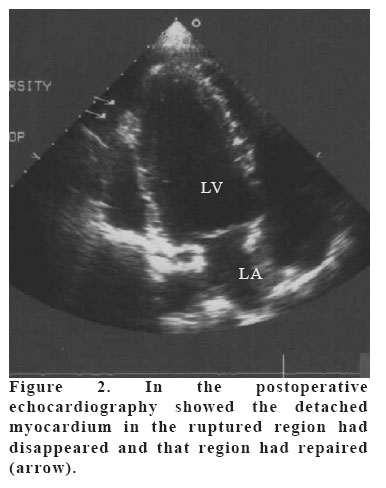
European Journal of General Medicine, Vol. 3, No. 1, 2006, pp. 41-44 A LETHAL BUT TREATABLE COMPLICATION: FREE WALL RUPTURE AFTER ACUTE MYOCARDIAL INFARCTION Mehmet S Ülgen1, Önder Öztürk2, Mehmet Kayrak1, Ahmet Soylu1, M Akif Düzenli1, Fatih Koç1 SelçukUniversity, Meram Medical Faculty1, Dicle University, Medical Faculty2, Department of Cardiology, Turkey Correspondence: M Sıddık Ülgen, MD, Selçuk Üniversitesi, Meram Tıp Fakultesi, Kardiyoloji AD, Konya, Türkiye Tel: 903322237039 E-mail: msulgen@hotmail.com Code Number: gm06009 A 43-year-old male patient was admitted to coronary intensive care unit with the diagnosis of acute inferolateral myocardial infarction and with a picture of cardiogenic shock. In physical examination, systolic blood pressure was 50 mmHg and diastolic blood pressure could not be taken. The patient was diagnosed with cardiogenic shock and was started on saline, dopamine and dobutamine infusion. His blood pressure did not increase although the dosage of positive inotropic agents was increased. A cardiac tamponade revealed with urgent echocardiographic evaluation and pericardiocentesis was carried out. Blood pressure returned to normal range within hours after pericardiosentesis. Echocardiographic examination performed on the second day of AMI on the asymptomatic patient revealed thrombosed myocardial rupture. The patient was referred to emergency surgery with the diagnosis of three-vessel disease and myocardial rupture according to urgent angiography. In the operation, the ruptured region in the ventricle free wall was primarily repaired. By-pass surgery was performed with saphenous vein graft to the LAD and CV-OM1 coronary arteries. Key words: Free wall rupture, acute myocardial infarction, treatment. INTRODUCTION Free wall rupture is the most lethal complication of acute myocardial infarction (AMI), and is responsible for about 10-15% of in hospital deaths (1-3). This rupture occurs most frequently in the left ventricular free wall, less frequently in the right ventricular free wall and rarely in the atrium. Early diagnosis and prompt treatment are essential in free wall rupture. But most are lost before the patient is referred to surgery. This paper presents a case of free wall rupture which led to a cardiac tamponade and cardiogenic shock in the course of AMI and was surgically repaired after his hemodynamics improved with urgent pericardiocentesis. CASE A 43-year-old male patient was admitted to coronary intensive care unit with the diagnosis of acute inferolateral myocardial infarction and with a picture of cardiogenic shock in the 5th hour of pain. In physical examination, systolic blood pressure was 50 mmHg and diastolic blood pressure could not be taken. Heart rate was 130/min, and there were signs of systemic hypoperfusion. In cardiac auscultation, heart sounds were tachycardic, regular and deep. Lung examination was normal. The patient was diagnosed with cardiogenic shock and was started on saline, dopamine and dobutamine infusion. The patient had a central venous pressure of 22 cm H2O and his blood pressure did not increase although the dosage of positive inotropic agents was increased and urgent echocardiography revealed a 1-cm pericardial effusion, causing a diastolic collapse of the right ventricle and containing coagulum. Urgent echocardiographic evaluation demonstrated cardiac tamponade and pericardiocentesis was performed and approximately 100 cc of hemorrhagic pericardial fluid was evacuated. Blood pressure returned to normal (120/70 mmHg) within 2 hours after the procedure and inotropic supportive treatment was tapered and stopped. Echocardiographic examination performed on the second day of AMI on the asymptomatic patient revealed that myocardium was transmurally detached in diameter of 0.5 cm in the apico-lateral region. There was a thrombosed appearance with fibrin structure in the epicardial part of the myocardium in the relevant region (Figure-1). Hypokinesia of the wall movements in the lateral and anterior basal walls was detected. Left ventricular ejection fraction was 50%. The case was recognized as a free wall rupture. Laboratory examination revealed a normal hemogram and routine biochemical parameters except for a typical increase in troponin CK-MB compatible with AMI. Urgent surgical intervention was planned with the diagnosis of free wall rupture according to the present findings. Coronary angiographies revealed 90% tubular narrowing in proximal left anterior descending(LAD), total occlusion in mid portion of circumflex artery(CX) and diffuse disease in right coronary artery(RCA) Ventriculography was not performed. The patient was referred to emergency surgery with the diagnosis of three-vessel disease and myocardial rupture according to angiography. During the operation, the ruptured region on the ventricle free wall was primarily repaired with pledget teflon felts. By-pass was performed with saphenous graft to the LAD and CX-OM1 coronary arteries. Postoperative period was without complications. Fifteen days after the operation, the dropout of myocardial appearance in the ruptured region had disappeared in the control echo and that region was repaired (Figure 2). DISCUSSION Free wall rupture after AMI is approximately 10 times less frequent than septum rupture and papillary muscle rupture (4). It is generally seen in the first 2 weeks and most frequently on the 3rd-5th days of infarction (5,6). Left ventricular rupture is 8 times more common than right ventricular rupture. It generally involves the anterior and the lateral walls of left ventricle. Rupture is mostly seen in the region joining the necrotic zone with the healthy tissue (7). Acute free wall rupture complicating acute myocardial infarction was defined as an abrupt and complete transmural rupture of the infracted region, causing cardiac tamponade and death in 30 minutes. Subacute rupture was defined as a gradual or incomplete rupture with slow or repetitive bleeding into the pericardial sac. In addition, Becker and van Mantgem have defined three types of ruptures (8). Type I: It is a sudden rupture in the left ventricle wall. Usually there is no thinning in the wall. Generally it appears in the first 24 hours and usually there is a one-vessel disease. Type II: There is an eroded region, thrombus and necrotic tissue together with a localized myocardial loss. It is an indication that the rupture is more subacute. Usually it occurs in multi-vessel patients. Type III rupture: It is usually in the form of aneurysm formation with myocardial thinning in a very large area and rupture in the middle of the aneurysm. This type of rupture also appears in the late phase. While the infracted region is of small or moderate size in Types I and II, in Type III there is rupture from the aneurysm which develops after extensive infarction. Free wall rupture is not related to infarct localizations. It is more frequently seen in first infarctions, women, above 60 years and especially in hypertensive patients without left ventricular hypertrophy (9, 10). Clinically, it is usually in the form of unexpected sudden death. Rarely, agitation, pain, vagal bradycardia, sinus tachycardia, nausea and restlessness can be observed a few minutes before death. Very rarely, transient hypotensive attacks and intermittent chest pain can be detected as preliminary findings (10). Sometimes it is possible to gain time until the operation in these ruptures which develop subacutely. The diagnosis of tamponade is made with echocardiography. Those with acute rupture cannot be saved except for rare cases. Two-dimensional echocardiography is important in early diagnosis (2, 11). If cardiac rupture is suspected on the basis of clinical symptoms and findings, a fast and sensitive diagnostic test to confirm myocardial rupture is transthoracic echocardiography. Echocardiography has increased the number of cases diagnosed before death and the number of surgical repairs attempted (12). Since direct signs of myocardial rupture were rarely identified by echocardiography, diagnosis of myocardial rupture was primarily based on the demonstration of hemopericardium and cardiac tamponade by echocardiography. Echocardiographic detection of intrapericardial high density echoes provides additional clues for myocardial rupture. In this case, it was accepted to be a Type I (acute) rupture because of localized myocardial loss and thrombus and 3-vessel disease in echocardiography. It is well known that diagnosis of free wall rupture complicating AMI is in itself an indication for emergency surgical intervention, irrespective of the clinical status of the patient. Because a major part of patients developing ventricular rupture die before a diagnosis is made, this lethal complication must be diagnosed and treated in the early period. Cardiac tamponade developing due to free wall rupture must be definitely ruled out in cases of severe hypotension or shock in the course of AMI. Therefore, the presence of an easily accessible echocardiography especially in intensive care units is of vital importance. In conclusion, early and detailed echocardiography can be life-saving in patients presenting with acute myocardial infarction and disturbed hemodynamics. REFERENCES
Copyright 2006 - Medical Investigations Society |

{kind=link}
{kind=link}