 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
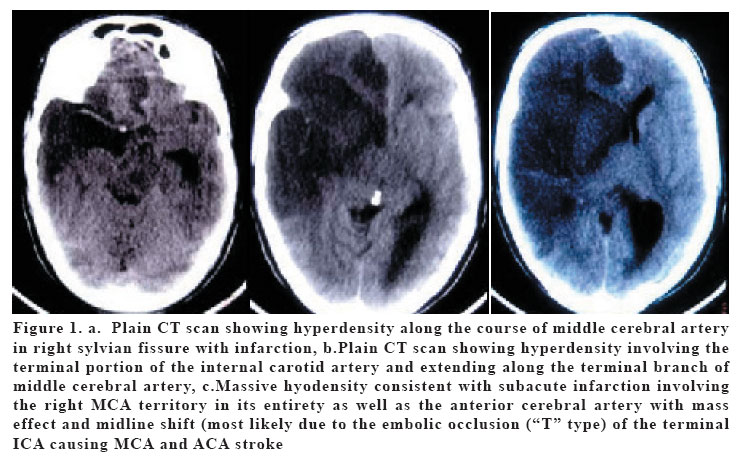
European Journal of General Medicine, Vol. 3, No. 1, 2006, pp. 45-47 AN ILLUSTRATIVE CASE OF HYPERDENSE MIDDLE CEREBRAL ARTERY SIGN Amit Agrawal1, Lekha Pandit2, Lathika Shetty3, Bobby Varkey3, Murali Manju1 K.S.Hegde Medical Academy, Departments of Neurosurgery1, Neurology2 and Radiology3 Mangalore, India Correspondence: Dr. Amit Agrawal K.S.Hegde Medical Academy, Department of Neurosurgery, Deralakatte-575018, Mangalore, India E-mail: dramit_in@yahoo.com Tel: 918242204472 Fax:918242204016 Code Number: gm06010 Hyperdense middle cerebral artery sign on non-contrast CT scan has been recognized as a marker of thrombus in the middle cerebral artery. It is associated with a subsequent large cerebral infarction and poor outcome despite treatment. This case illustrates the sign and also its grave consequences. Key words: Infarction, middle cerebral artery, malignant middle artery syndrome, stroke INTRODUCTION The management of ischemic stroke has improved greatly over the past two decades in terms of stroke treatment and there is strong evidence that outcomes after stroke can be improved and that death or disability from stroke can be reduced with appropriate treatment. However, in some cases where infarction involves the entire middle cerebral artery (MCA) territory can cause “malignant” MCA infarction with resultant fatal outcome (1-3). We discuss an illustrative case of malignant MCA infarction with characteristic hyperdense middle cerebral artery sign on plain CT scan and review the relevant literature. CASE A 35-year-old right handed gentleman from rural south India presented with sudden onset of left sided weakness of 1 day duration and multiple episodes of left focal seizure with secondary generalization following that he lapsed into altered sensorium. He was a known hypertensive for last 8 years on regular medication. On examination his blood pressure was -130/90 mmHg and other general and systemic examination was normal. Neurologically GCS was E1V1M3 with left sided weakness. Both the pupils were dilated and fixed and extra-ocular movements were frozen. There was generalized hypertonia with bilateral extensor plantars. Blood investigations were normal except mild leucocytosis (Total count-18,400) and raised ESR of 10 mm/h. Non-contrast CT scan of brain showed hyperdensity involving the terminal portion of the internal carotid artery and extending along the course of right middle cerebral artery in the sylvian fissure also involving one terminal branch with massive cerebral infarction and oedema causing midline shift (anteroseptal and pineal shift), obliteration of the right lateral ventricle and dilatation of the left lateral ventricle and temporal horn of the lateral ventricle (Figure 1). In spite of aggressive management the patient expired on third day after admission. DISCUSSION The recognition of hyperdensity in the distal MCA and its branches in the sylvian fissure (Hyperdense middle cerebral artery sign; HMCA sign) on non-contrast CT scan has been recognized as a marker of thrombus in the middle cerebral artery and a harbinger of a subsequent large cerebral infarction and poor outcome (1-3). The incidence of the HMCA sign on CT scans varies from 5%-41% and only one fifth of patients with this sign have an excellent prognosis (4,5). Identification of the HMCA sign has been shown to have a high positive predictive value for detection of middle cerebral artery thrombus on an arteriogram however the reliability of this sign is uncertain particularly in the elderly where thrombosis can be confused with calcified artery walls (6,7). As this case also illustrates presence of the HMCA sign identifies a group of patients who do more poorly than those not exhibiting the HMCA sign on non-contrast CT scan. This malignant middle cerebral artery syndrome occurs in 10% to 15% of supratentorial infarction cases and involves the entire middle cerebral artery (MCA) territory. This “malignant” MCA infarction suffers from progressive clinical deterioration because of increasing brain swelling, raised intracranial pressure (ICP), and brain herniation (8). Large multicentre trials and studies provide many evidences of the value of intravenous thrombolysis with rtPA, anticoagulants, antiplatelet agents, and so on. There is strong evidence that outcomes after stroke can be improved and that death or disability from stroke can be reduced with appropriate treatment (9,10). Despite these advances malignant middle cerebral artery (MCA) infarction is associated with mortality rate of up to 80% (11,12). This patient subpopulation constitutes a particularly difficult challenge and considering the fact this is associated with high mortality yielded by conservative treatment, therapy of malignant MCA infarction should be more aggressive (11,12). The role of surgical decompression in malignant MCA infarction is still controversial and needs to be clearly defined further. Decompressive craniectomy with durotomy is usually performed as a last resort in patients with malignant brain edema because of infarction or trauma (9,13). Decompressive surgery can reduce ICP, secondary ischemia, edema and can also significantly decrease infarction size. However, this procedure can allow bulge of brain tissue through the defect. This frequently results in compression of vessels by the dural margin with further congestion, edema, ischemia and hemorrhage in the bulged brain tissue (11). Decompressive craniectomy in younger patients with malignant MCA territory infarction improves both survival rates and functional outcomes. Although survival rates are improved after surgery in elderly patients, functional outcome and level of independence is poor (11). REFERENCES
Copyright 2006 - Medical Investigations Society |

{kind=link}