 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
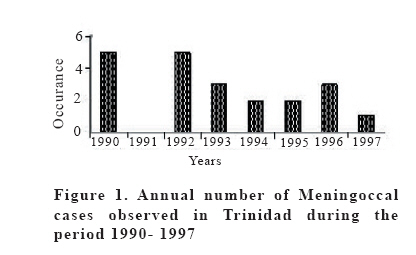
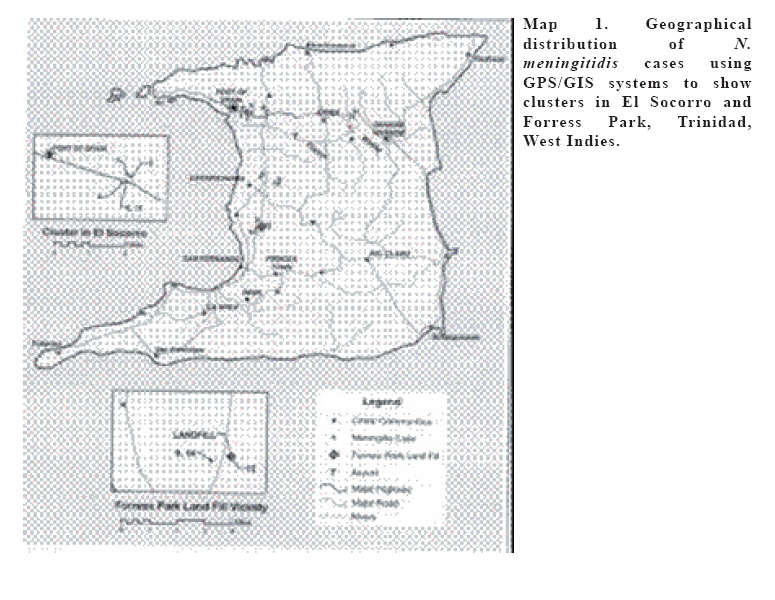
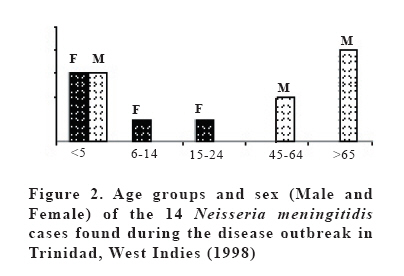
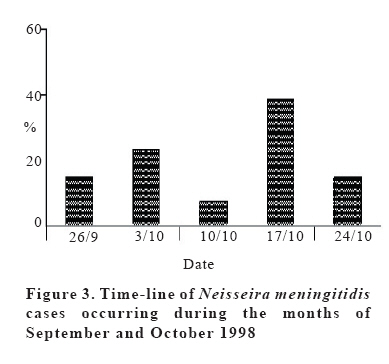
European Journal of General Medicine, Vol. 3, No. 2, 2006, pp. 49-53 MENINGOCOCCAL MENINGITIS OUTBREAK IN TRINIDAD, 1998 Dave D. Chadee1, Robert Lee2, Anthony Ferdinand3, Parimi Prabhakar2, Denise Clarke2, Benjamin Jacob4 University of the West Indies,1Department of Life Sciences, St. Augustine, 2Caribbean Epidemiology Centre, Federation Park, Port of Spain, University of the West Indies, 3Department of Para Clinical Studies, Faculty of Medicine, Mt. Hope, Trinidad and University of Miami School of Medicine, 4Department of Epidemiology and Public Health, Miami, Florida, USA Correspondence: Dr D.D. Chadee , Department of Life Sciences, University of the West Indies, St. Augustine Trinidad, West Indies Phone-1-868-645-3232-7 Ext. 3740 Fax: 1-868-663-6129 E-mail:chadee@tstt.net.tt Code Number: gm06011 Aim: To describe an outbreak of serogroup B neisseria meningitidis occurred in Trinidad during 1998. Keywords: Neisseria meningitidis, serogroup B outbreak, mortality, GPS/GIS, surveillance, Trinidad INTRODUCTION The World Health Organization (WHO) estimates that 1.2 million cases of bacterial meningitis occur annually, with 135,000 deaths, making it a major cause of morbidity and mortality in both developed and developing nations. Neisseria meningitidis is the etiological agent in more than 40% of these cases (1). The African meningitis belt, which stretches from Senegal to Ethiopia, has the highest incidence of the disease, but N. meningitidis is also responsible for recent outbreaks in Asia and the Americas (2,3). Serogroup A has caused the majority of the African epidemics (4) while Serogroup C has caused outbreaks in North America as well as in Africa. However, serogroup B has caused sporadic outbreaks in South American and the Caribbean, including Cuba (1982-1984), Chile (1986, 1993), Brazil (1988) and other parts of the world (4). Meningitis is endemic in many countries in the Caribbean region, with causative agents varying from serogroup B Streptococcal meningitis in Trinidad and Cuba (5,6,7) to Hemophilus influenzae in Jamaica (8). In Trinidad, Streptococcal meningitis was found to be a very common clinical presentation (44%) whereas neonatal meningitis prevalence was found to be extremely low with 0.28% (49/17048) (5,6). Trinidad and Tobago (population 1.2 million) generally has a low occurrence of meningococcal meningitis with only occasional isolated cases. From 1990 to 1997 there was an average of 3 confirmed cases per year (Figure 1) but these cases were geographically isolated with no epidemiological clusters. During September- October 1998 a meningococcal outbreak occurred in Trinidad and this paper reports on the epidemiologic features of this outbreak of N. meningitidis serogroup B in Trinidad in 1998. MATERIALS AND METHODS Background The island of Trinidad is located approximately 110 North, 15 km from the east coast of Venezuela, from which it is separated only by the shallow Gulf of Paria (Map 1). The island is roughly rectangular in shape, with large promontories on the northwest and southwest and an area of circa 4662 km2. The island’s greatest length is 90km, from north to south, and its greatest breadth is 57.6 km, from east to west. It has a population of about 1.2 million (9). The case definition for confirmed cases was an isolate of N. meningitidis and consistent symptoms of meningitis including petechial rash in association with sudden onset of fever, headaches and stiff neck. The case definition for suspected cases was symptoms of headache, fever and stiff neck, with an absence of an isolate of N. meningitidis and no other obvious explanation for the observed symptoms. Case Investigations Following the identification of the first case of N. meningitidis a thorough investigation was conducted by a team of Epidemiologist, Medical Officers, Surveillance Nurses and District Health Visitors to determine the case distribution within the community including schools. From the end of September to December 1998 epidemiological studies were initiated including contact tracing, swabbing of the immediate family of all cases and neighboring household, and the provision of prophylactic treatment (Rifampicin) to all contacts and surveillance workers. All positive isolates were sent to the Laboratory Centre for Disease Control (Federal Laboratories), Bureau of Microbiology, Winnipeg, Manitoba, Canada for serogroup typing. During the outbreak, the location of every case was determined using a GPS (Trimble GeoExporer: Trimble Navigation, Sunnyvale and Garmin GP 45: Garmin International, Inc. Olathe, KS). Precise coordinates of all cases were entered into a GIS (ArcView, ESRI, Redlands, CA), and associated with attribute data of N. meningitidis. A spatial distribution map was produced using ArcView GIS. RESULTS On 1st October 1998, a five year old boy who lived in Forress Park, Claxton Bay, was admitted to Port of Spain General Hospital and died within 24 hours of admission. A cerebral spinal fluid sample was sent to the Trinidad Public Health Laboratory and the Caribbean Epidemiology Centre for bacteriological testing. From the CSF sample Neisseria meningitidis serogroup B was isolated thus corroborating the diagnosis at post-mortem. Upon investigation, it was revealed that the child lived in close proximity to a sanitary landfill site in Claxton Bay (Map 1). Swabs taken from the mother of the child were found positive with N. meningitidis serogroup A, but she was asymptomatic suggesting a “carrier” status. On further investigation an employee of a bakery in El Socorro, San Juan, Trinidad, died on 26th September 1998. The owner of the bakery was found to be an asymptomatic “carrier” while his brother died 48 hours earlier falling victim to a similar infection and dying within 24 hours of admission to the St. Clair Medical Centre. Nasopharyngeal swabs were taken and demonstrated the presence of N. meningitidis serogroup B. The owner of the bakery is considered the index case but a “carrier”. Twenty-one cases of suspected N. meningitidis were reported to the Trinidad Public Health Laboratory between 26th September and 10th December 1998. All cases were hospitalized. Fourteen cases were subsequently confirmed as N. meningitidis by bacterial culture. Figure 2 shows the sex and age distribution of the 14 confirmed cases, with the most significant age group contracting N. meningitidis being <5 with 42.9%, followed by the 45-64 age group with 28.6%. Overall, there was a 57.1% (8 cases) mortality rate among the 14 cases detected. The mortality rate was highest among the <5 year old with 50% (4 cases), followed by age groups 24-44 (2 cases) and 45-64 (2 cases) with 25% respectively. No deaths occurred among the other age groups. The epidemiological curve or timeline indicated that over 38% of the cases were detected on the 17th October 1998 (Fig.3). Eleven cases were clustered from 3rd October to 24th October 1998 and had in common persons working, purchasing items or living in close proximity to the bakery in the town of El Socorro, Trinidad (See Map 1) An investigation on the linkage between the cases in El Socorro and the first case in Claxton Bay revealed that a garbage truck from opposite the bakery frequently transported materials to the dump at the Forress Park sanitary landfill in Claxton Bay. The other two cases, one of serogroup A and the other of serogroup B, were observed from other geographical locations and had no obvious factors linking them to the above cases. The georeferenced database was used to calculate spatial distance between N. meningitidis cases and revealed two epidemiological clusters, one in El Socorro and the other in Forress Park, Claxton Bay, Trinidad (Map 1). DISCUSSION The small outbreak of N. meningitidis in Trinidad can be attributed to numerous factors, many of these factors are not fully understood, but a complex combination of host, agent and environmental risk factors appear to be involved. Results from Figure 1 showed that an average of 3 cases of meningitis is observed annually in Trinidad. These results suggest that N. meningitidis is endemic and maintained by “carriers” who made up over 28% of the cases identified during this outbreak. These results are consistent with carrier levels (25%) observed in the meningitis belt (10). It has been reported that N. meningitidis serogroup B is commonly asymptomatic in the Americas and is not usually associated with clusters of cases but rather gives rise to sporadic cases (7,11)). However, the present outbreak was caused by serogroup B which suggests a possible change in pathogenicity or a recent introduction of a new pathogenic strain. Some environmental factors such as low humidity, high temperature and dust have been suggested as factors for enhancing meningococcal invasion by directly damaging the mucosal barrier or by inhibiting mucosal immune defenses (12). The identification of four cases associated within a dusty sanitary landfill site supports the hypothesis that living, working and playing at such sites are risk factors. It is clear that although factors which predisposed a population to N. meningitidis are poorly understood, population susceptibility, introduction of new strains or “carriers”, poor living environment, adults scavenging among contaminated materials at the dump, dusty environment and concurrent infections have been implicated (11,12,13, present study) The primary mode of transmission of the current outbreak was possibly by direct contact, including droplets and discharges from nose and throat of infected persons. Infection is likely to have occurred from contact with “carriers’ identified during the outbreak investigation. The transmission to family, employees of the bakery and residents from the surrounding areas possibly occurred by contact with droplets while purchasing items or within the home. It is hypothesized that the infectious agent was transported from El Socorro to Forress Park via the garbage truck which dumped the potentially hazardous material at the landfill site (Map 1). An important element of this meningitis outbreak was the fact that the brother of the index case sought immediate medical attention which coincided with the bacterial isolation of N. meninigitidis from CNS fluid of the second case from Forress Park. So after the first diagnosis of meningitis, the disease response time to the emergency was short and the 20 other suspected cases in El Socorro, Forress Park, Couva and Curepe were found and hospitalized within 10 days, thanks to a cadre of well trained Ministry of Health staff. The speed of this response possibly averted a large scale meningitis outbreak in El Socorro and Forress Park and its proliferation to other parts of the island. The results of this study also demonstrated the usefulness of active surveillance after a case is detected, for without the extension of the survey into Valencia along the east west corridor, the 14th case, would not have been discovered. Mapping of the current spatial distribution of the outbreak highlighted the importance of county-level surveillance in Trinidad and Tobago. In addition, it supports the development of improved surveillance systems by identifying essential monitoring regimens, both within and at the periphery of outbreak-sample areas. For example, if the periphery of the outbreak areas were not monitored, cases in Valencia and Curepe would not have been detected. The application of the GIS provided a visual confirmation of the N. meningitidis outbreak showing two distinct clusters, one in the north and the other in south central Trinidad. It is clear that the usefulness of the geographic information systems will allow for the rapid production of maps and will assist in identifying clusters and in directing the necessary resources for the epidemic response. The results of this study suggest that further studies should be conducted near sanitary landfill sites to determine the prevalence of N. meningitidis and to better understand the environmental risk factors for meningitis in Trinidad and Tobago and the wider Caribbean region. Acknowledgements We wish to thank all the Nurses from County medical Officers of Health Departments in St. George Central and Caroni for their expert assistance during the cases investigations. We also thank the laboratory staff at the Trinidad Public Health Laboratory and the Caribbean Epidemiology Centre for dedicated service and finally we thank Ms. C.A. Campbell, Smith College, Northampton, Mass. USA for assistance during the preparation of the manuscript. REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06011f2.jpg] [gm06011f1.jpg] [gm06011f4.jpg] [gm06011f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}