 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
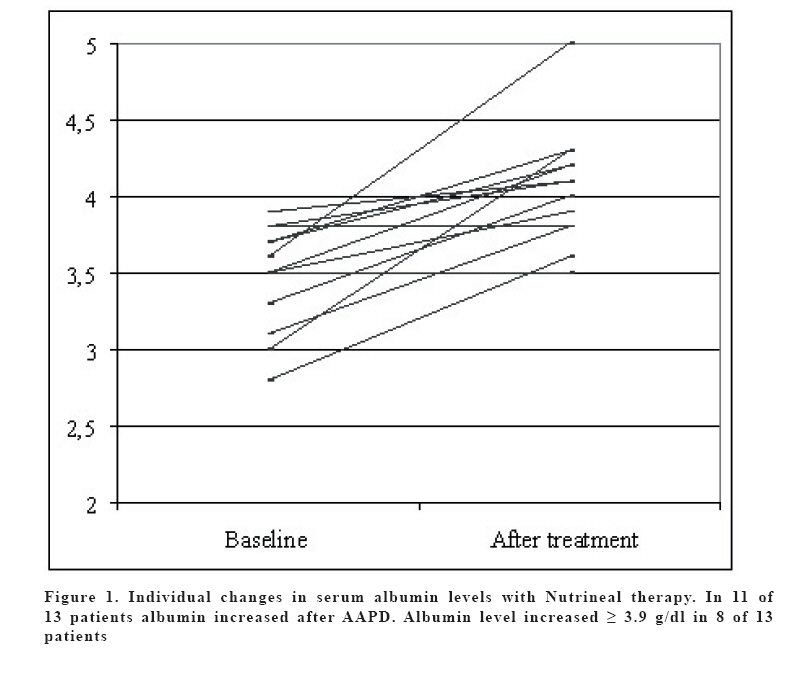
European Journal of General Medicine, Vol. 3, No. 2, 2006, pp. 58-63 EFFECTS OF AMINO ACID PERITONEAL DIALYSATE IN MALNUTRISHED PERITONEAL DIALYSIS PATIENTS Mehmet Tugrul Sezer 1, Murat Demir 1, Jale Ertürk 1, Mustafa Yildiz 2 Süleyman Demirel University, Faculty of Medicine, Division of Nephrology, Departments of Internal Medicine1 and Nuclear Medicine2, Isparta, Turkey Correspondence: Dr. Mehmet Tugrul Sezer Süleyman Demirel Universitesi, Tıp Fakültesi, İç Hastalıkları AD, Doğu Kampüsü, Isparta, Türkiye Phone: 902462112887, Fax: 902462371165 E-mail: tugrul@med.sdu.edu.tr Code Number: gm06013 Aim: Malnutrition is common in peritoneal dialysis (PD) patients and hypoalbuminemia is a predictor of poor outcomes in end-stage renal disease patients. Amino acid peritoneal dialysate (AAPD) is used to improve nutritional status in malnourished PD patients. In this study, we investigated effects of AAPD on nutritional parameters in hypoalbuminemic PD patients. Key words: Albumin, HDL cholesterol, malnutrition, nutritional assessment, peritoneal dialysis INTRODUCTION Malnutrition is associated with reduced protein-energy intake and has many effects on the clinical condition (1). It is well documented that protein-energy malnutrition is common among patients with chronic renal failure (CRF) (2, 3). The prevalence of malnutrition is reported to be 40-54% in peritoneal dialysis (PD) patients (4-6). The etiology of malnutrition in CRF is complex and includes many factors such as poor food intake, inflammation, gastrointestinal symptoms (nausea and vomiting), metabolic acidosis and increased resting energy expenditure. Malnutrition is also an important risk factor for morbidity and mortality in end stage renal disease (ESRD) patients (2, 3). Several biochemical markers (serum albumin, prealbumin, transferrin etc.), semiquantitative method of subjective global assessment (SGA) (7), malnutrition-inflammation score (8) and lean body mass (LBM) by dual X-ray absorptiometry (DEXA) have been used for evaluation of nutritional status. Amino acid peritoneal dialysis (AAPD) solutions have been used in PD patients to improve nutritional status. In hypoalbuminemic PD patients, some studies showed that serum albumin levels increased with AAPD solution (9, 10) but others not (11). Therefore, we investigated the effects of AAPD on nutritional status in hypoalbuminemic PD patients. MATERIAL AND METHODS Study design This is a prospective, open label, uncontrolled study. The Ethical Committee of Süleyman Demirel University approved the study. After informed consent was obtained, the patients recruited for the study. During the study period, one dextrose peritoneal dialysate exchange was replaced every noon by a 2-L AAPD. The usual dwell time of AAPD was 5-6 hours. The dwell times and volumes were not changed during the study period. After three months period, biochemical and other nutritional parameters were measured again to compare with baseline parameters. Patients We studied 16 (10 male and 6 female) prevalent patients with ESRD on continuous ambulatory peritoneal dialysis (CAPD). At the beginning of the study, demographic and clinical characteristics of the patients were recorded. Demographic characteristics of the patients are shown in Table 1. If the patient serum albumin level was with persistently ≤3.9 g/dL despite repeated dietetic consultation, they were included into the study. Patients were excluded, if they had an episode of peritonitis within last three months, hospitalized within 3 months or had a concomitant disease that could have led to a catabolic state. Nutritional assessments and examinations As nutritional parameters, serum albumin level, SGA, n-PCR and LBM measured by DEXA were used. At the baseline, the patients were assessed for these nutritional parameters. After an overnight fasting, blood samples for serum albumin, lipid parameters, high sensitive C-reactive protein (s-CRP) were drawn from antecubital vein. All patients blood samples were drawn when they were normovolemic and without inflammatory status present. Biochemical parameters were measured in our central laboratories. Serum albumin was measured with bromocresol purple method. (normal range in 3.4 to 4.8 g/dL). For detection of serum s-CRP chemiluminescent-based method was used. SGA was done as defined elsewhere (7) for each patient by a renal nurse (JE). Total body LBM was measured by DEXA in the Norland XR-46 bone densitometer (with dynamic filtration, Norland Corp, Fort Atkinson, USA). The Norland XR-46 was calibrated daily, 30 minute after turning the apparatus on. Peritoneal Adequest 2.0 (Baxter) program was used to measure n-PCR as defined before (12). Weekly Kt/Vurea was performed to evaluate peritoneal function and creatinine clearance (CCr) was performed to evaluate residual renal function before and three months after AAPD treatment. Statistical analysis The results were expressed as means ±SD. Differences between baseline and after treatment parameters were analyzed with Wilcoxon signed rank test and P value less than 0.05 was considered statistically significant. Spearman correlation test was used for correlation analysis RESULTS During the study period two patients dropped out due to bacterial peritonitis and one patient due to intermittent diarrhea. The reasons of the peritonitis were contamination in one and unknown in other. Non-infectious diarrhea developed in a patient with amyloidosis, but this patient was suffering from intermittent diarrhea even before the study and it was thought to be due to amyloidosis. These three patients did not complete the study and were excluded from the statistical analysis. Thirteen patients completed the study. Baseline and after treatment, laboratory parameters are shown in Table 2. After three months of AAPD usage in these hypoalbuminemic CAPD patients, serum BUN and albumin levels, n-PCR and SGA values increased, but HDL cholesterol and 24 hour urine creatinine clearance decreased. The changes in LBM were not statistically significant. Individual changes in serum albumin levels are shown in Figure 1. Overall serum albumin increased from 3.5 ± 0.5 g/dL to 4.1 ± 0.4 g/dL (P=0.003) in 11 of 13 patients (84 %) and in seven of thirteen patients (53 %) serum albumin increased over 4g/dL. In two patient baseline and after treatment, serum albumin values were the same. In this study, in 10 of 13 (73%) patient baseline serum s-CRP levels were lower than 1 mg/dL (range 0.06 mg/dL to 0.73 mg/dL) and baseline serum s-CRP levels were higher than 1 mg/dL only in three patients (23%) (range 1.11 mg/dL to 4.25 mg/dL). Eight of thirteen patients (61%) were anuric. In five patients CCr ranged between 0.1 ml/min to 14.0 ml/min. When five patients with residual renal function were assessed CCr was 5.07 ± 6.16 ml/min before treatment and 2.81 ± 3.48 ml/min (P=0.04) after treatment. After treatment, HDL cholesterol level decreased from 43.1 ± 7.3 mg/dL to 37.8 ± 6.0 mg/dL (P=0.02), even though other lipid parameters (total cholesterol, triglyceride and LDL cholesterol) did not change. Correlations Among baseline parameters, there was a positive correlation between BUN and albumin (r=0.62 P=0.02), between BUN and nPCR (r=0.66 P=0.01), and a negative correlation between hemoglobin and s-CRP level (r=-0.72 P=0.01). Also among after treatment parameters, there was a positive correlation between SGA and albumin level (r=0.69 P=0.008). DISCUSSION In this study, we showed that AAPD could be used to improve nutritional status in PD patients whose serum albumine level were ≤3.9 g/dL. Studies about efficacy of AAPD in malnourished PD patients have given conflicting results (9-11). Therefore, the aim of this study was to investigate the effects of AAPD on nutritional status of CAPD patients with serum albumin level ≤3.9 g/dL. Recently a link between malnutrition, inflammation and atherosclerosis namely MIA syndrome had been defined (13, 14). We used serum s-CRP level as an inflammation marker. In this study, all patients tolerated the AAPD well. No patient suffered uremic symptoms described in other studies (9, 15). One patient with amyloidosis experienced non-infectious diarrhea that was also present prior to study. During the study period, bacterial peritonitis developed in two patients. Li et al (16) reported that, peritonitis incidence was lower in patients using AAPD than in patients using glucose solution, but not statistically significant. We believe that these episodes were coincidental and not due to use of AAPD. Dietetic consultation, anabolic agents (insulin-like growth factor-1) and AAPD are the strategies for malnutrition management in PD patients. Newer PD solutions are designed to manage comorbidities associated with patients on maintenance dialysis and to better preserve peritoneal membrane function and host defenses. The evidence to date indicates that, in malnourished PD patients AAPD solutions improve protein nutritional status, particularly if low protein intakes are a cause of the malnutrition (17). APD containing 1.1% amino acids as the osmotic agent, was developed to control malnutrition in these patients (18, 19). Some studies had demostrated that, AAPD was an effective agent to improve nutritional status in malnourished PD patients (9, 10). On the other hand, Misra et al (11) reported that there was no significant increase in serum albumin with AAPD in well-nutrished patients. As most of the currently published studies, the duration of this study was three months. In this study, in 11 of 13 patients (84 %) serum albumin level increased after treatment. Likewise albumin, other nutritional parameters including BUN, nPCR and SGA increased. Also this suggests that, AAPD not only increases serum albumin level and also it improves nutritional status in hypoalbuminemic patients. Despite the increas of BUN level after treatment, none of the patient suffered from nausea or vomiting. Inflammation is one of the causes of hypoalbuminemia in ESRD patients. Stenvinkel et al reported the association between hypoalbuminemia and inflammation (13). Baseline s-CRP levels were found lower than 1 mg/dL in 10 of 13 patients (77%) and higher than 1 mg/dL in three patients (23%). Mean serum albumin increased only 0.2 g/dL (range 0 to 0.4 g/dL) in patients with s-CRP higher than 1 mg/dL. However in patients with s-CRP lower than 1 mg/dL, serum albumin increased as an average by 0.6 g/dL (range 0.3 to 1.4 gr/dL) after treatment. We believe that because of low inflammatory status, effect of AAPD on serum albumin level were evident in our patients. However there was no significant correlation between baseline serum s-CRP and albumin (r=0.46 P=0.17). There was a positive correlation between baseline values of BUN and albumin. In addition there was a positive correlation between SGA and albumin after treatment. These correlations between nutritional parameters suggest that increase in serum albumin level is related to other nutritional parameters. AAPD not only increased serum albumin level, but also improved other nutritional parameters. On the other hand, unchanged LBM by DEXA might be due to short treatment duration and the small number of patients. Only five of 13 patients (38%) had a residual renal function. In these five patients, basaline CCr was 5.07 ± 6.16 ml/min at baseline. After three months of AAPD usage, CCr was decreased 2.81±3.48 ml/min in these five patients. We can not speculate whether this dramatic decrease in CCr is due to the use of AAPD or progression of renal parenchymal disease. Misra et al (20) investigated the effects of AAPD on lipid metabolism in PD patients and found that, the use of AAPD in hyperlipidemic PD patients with serum cholesterol ≥ 5.5 mmol/L is safe. Also they did not report any side effect of AAPD on lipid metabolism in hyperlipidemic PD patients. However in our patients HDL cholesterol decreased after the use of AAPD. Yang et al (21) reported that serum homocysteine level increased and HDL cholesterol decreased after three months AAPD usage in their patients. This is the second study reporting that HDL cholesterol decreased but total cholesterol, triglyceride, and LDL cholesterol did not change significantly after a short time AAPD usage in hypoalbuminemic CAPD patients. Limitations of our study; its uncontrolled nature, the small number of the patients and the short duration. We did not measure serum bicarbonate level at baseline and after treatment. In conclusion, our data suggest that AAPD could be used as an effective agent to improve nutritional status in hypoalbuminemic PD patients. Despite the observed positive effects on nutritional parameters, the mechanism of HDL cholesterol decrease and the dramatic decrease in CCr should be investigated in further studies.
REFERENCES
Copyright 2006 - Medical Investigations Society The following images related to this document are available:Photo images[gm06013t2.jpg] [gm06013f1.jpg] [gm06013t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}